Bloating and gas while you are still eating can happen when swallowed air, fast eating, carbonated drinks, high-fermentation foods, delayed stomach emptying, constipation, or gut-brain sensitivity create pressure before the meal is finished. Pattern tracking matters because the trigger is not the same for everyone.
How did we evaluate bloating and gas while eating?
We evaluated this question by separating common physiology from red-flag symptoms and supplement marketing. NIDDK, Mayo Clinic, and Cleveland Clinic references received more weight than anecdotal forum explanations because they distinguish swallowed air, fermentation, constipation, motility, and medical evaluation. We excluded claims that one food, one test, or one supplement explains every bloating pattern. The main limitation is that bloating is a symptom description, not a diagnosis, so the safest answer focuses on timing, meal context, stool pattern, and clinician review when symptoms are severe, new, or persistent.
Why can bloating start before a meal is finished?
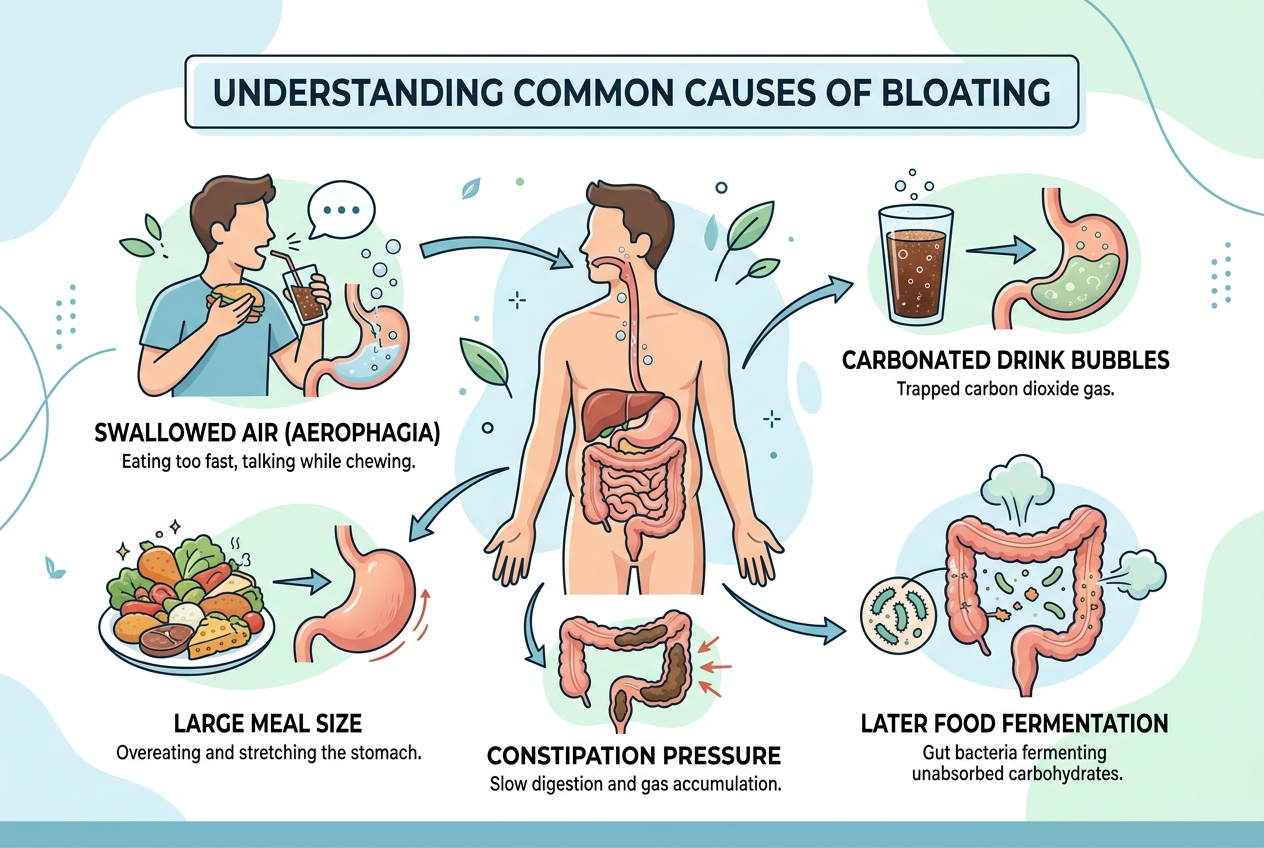
Bloating can start during a meal because the digestive tract responds before food reaches the colon. Swallowed air enters the stomach when a person eats quickly, talks while chewing, drinks through a straw, chews gum, or uses carbonated drinks. The NIDDK explains that gas comes from swallowed air and bacterial breakdown of carbohydrates. Stomach stretching can also create pressure signals during a large meal, especially when fat, alcohol, or stress slows normal movement. Some people feel pressure earlier because visceral hypersensitivity makes ordinary gas or stretching feel more intense. Fermentable carbohydrates usually create more gas later, but meal timing can overlap when breakfast, lunch, snacks, and constipation keep the gut already loaded. The key clue is timing: immediate pressure points toward air, stomach distension, or sensitivity, while delayed gas points more toward fermentation.
What meal patterns make immediate bloating more likely?
Immediate bloating becomes more likely when meal speed, volume, beverage choice, and food texture increase stomach pressure. Large meals stretch the stomach more than smaller meals, and carbonated beverages add gas directly before digestion begins. High-fat meals can slow gastric emptying, so pressure can linger longer after the first bites. Wheat, onions, beans, apples, milk, sugar alcohols, and some protein bars can add fermentable carbohydrate load, although fermentation usually shows up later. The NIDDK IBS diet guidance notes that certain carbohydrates can trigger gas and bloating in sensitive people. Constipation also matters because stool retention can reduce room in the colon and make normal meal-related reflexes feel stronger. A useful pattern log records meal size, eating speed, carbonation, dairy, wheat, onions, beans, stool frequency, and symptom timing.
How can you tell swallowed air from food fermentation?
Swallowed air usually creates upper-abdominal fullness, burping, pressure, or discomfort during the meal or shortly afterward. Food fermentation usually creates lower-abdominal gas, rumbling, flatus, or distension several hours later, although overlapping meals can blur that timeline. Mayo Clinic describes gas and gas pains as common and often related to swallowed air or food breakdown, but persistent or severe symptoms deserve evaluation (Mayo Clinic). The practical test is not perfect, but it is useful: slow the meal, skip carbonation, avoid straws, and eat smaller portions for several days. If immediate pressure drops, swallowed air or stomach distension was probably part of the pattern. If symptoms remain tied to specific carbohydrates hours later, fermentation or intolerance becomes more plausible. If stool frequency is low, constipation can amplify both patterns.
What should you track before changing your diet?
Track timing, location, stool pattern, meal details, and repeatability before removing broad food groups. A simple two-week log should record the first symptom minute, upper versus lower pressure, burping, flatus, stool frequency, stool form, carbonation, meal speed, dairy, wheat, onions, beans, garlic, fruit, protein powders, and sugar alcohols. Cleveland Clinic notes that bloating can reflect gas, digestive contents, or visceral sensitivity, and evaluation depends on the pattern (Cleveland Clinic). The goal is to find a reproducible signal, not to create a fear list. Change one variable at a time: meal pace, carbonation, portion size, lactose, or high-FODMAP foods. A broad elimination diet can hide the actual trigger and make eating more stressful. A log also helps a clinician decide whether testing for lactose intolerance, celiac disease, constipation, reflux, or other causes is reasonable.
When is bloating while eating worth medical attention?
Bloating while eating is worth medical attention when it is new, worsening, severe, persistent, or paired with warning signs. Red flags include vomiting, blood in stool, black stool, fever, unexplained weight loss, progressive trouble swallowing, persistent diarrhea, severe pain, anemia, or symptoms that wake someone at night. People with pregnancy, immune compromise, recent abdominal surgery, inflammatory bowel disease history, or major medication changes should also use a lower threshold for care. Most meal-related gas is not an emergency, but repeated early fullness can sometimes point to motility issues, constipation, reflux patterns, or other conditions that need evaluation. A clinician can review diet logs, stool patterns, medications, and basic tests without guessing from one symptom. The safest rule is simple: mild and pattern-based symptoms can be tracked; intense or escalating symptoms should be assessed.
What practical steps can reduce bloating during meals?
Start with low-risk changes that reduce air, pressure, and overload. Eat more slowly, chew fully, avoid straws, pause carbonated drinks, and reduce very large meals for one week. Keep posture upright during and after meals, and avoid stacking heavy snacks close together if symptoms appear before dinner. If constipation is present, address stool regularity with hydration, fiber tolerance, movement, and clinician guidance rather than only removing foods. If lactose seems likely, compare lactose-containing and lactose-free meals without changing five other variables. If high-FODMAP foods seem likely, use a structured approach rather than permanent restriction. These steps do not diagnose the cause, but they make the pattern easier to read. If the pattern points toward supplement comparison later, a separate buying guide can compare digestive support options without replacing medical evaluation.
What questions do people ask about bloating while eating?
Can gas happen before food reaches the colon?
Yes. Swallowed air can create gas pressure in the stomach during the meal. Fermentation usually happens later, but overlapping meals and constipation can make timing confusing.
Does immediate bloating mean a food intolerance?
Not automatically. Immediate bloating can reflect air swallowing, carbonation, meal size, stomach stretching, stress physiology, or sensitivity. A repeatable pattern is stronger evidence than one uncomfortable meal.
Can eating too fast cause bloating?
Yes. Fast eating can increase swallowed air and make large portions easier to overeat. Slower meals are a low-risk first test.
Should I cut out gluten first?
Not without a reasoned pattern or clinician guidance. Gluten, wheat fructans, meal size, carbonation, lactose, and constipation can create similar symptoms, so broad restriction can confuse the signal.
Can constipation make meals feel bloating sooner?
Yes. Constipation can increase baseline pressure and make normal meal reflexes feel stronger. Stool frequency and stool form belong in the symptom log.
What if bloating happens with severe pain?
Severe pain, vomiting, blood, fever, weight loss, or worsening symptoms should be evaluated. A self-tracking plan is not enough for red-flag patterns.
What is the bottom line?
Bloating and gas while eating usually needs pattern analysis, not panic. Start by reducing swallowed air, carbonation, large meals, and rushed eating while tracking stool pattern and symptom timing. If the pattern persists, worsens, or includes red flags, bring a two-week log to a clinician instead of guessing from one meal.
Leave a Reply