Visible bloating with negative tests can come from abdominal wall coordination, gas sensitivity, constipation, food triggers, or gut-brain interaction patterns. Forcing the abdomen outward may mimic or worsen distension, but it should not be self-diagnosed as the only cause. Track posture, breathing, meals, stool pattern, and red flags before changing treatment plans.
How did we evaluate bloating with negative tests?
We evaluated this question by separating abdominal bloating, which is a sensation of pressure or fullness, from abdominal distension, which is a visible or measurable increase in abdominal size. Reviews on abdominophrenic dyssynergia, NIDDK patient guidance, Mayo Clinic professional guidance, and randomized biofeedback research received more weight than anecdotal posture explanations. We excluded claims that one breathing pattern explains every long-term bloating case, because constipation, carbohydrate intolerance, pelvic floor dysfunction, medication effects, and gynecologic conditions can overlap. We prioritized explanations that a patient could observe without making a diagnosis at home. We also treated negative tests as context, not as proof that symptoms are imaginary. The main limitation is that “all tests negative” can mean different test panels, so persistent, worsening, painful, or new distension still deserves clinician review.
Can forcing the abs outward make bloating look worse?
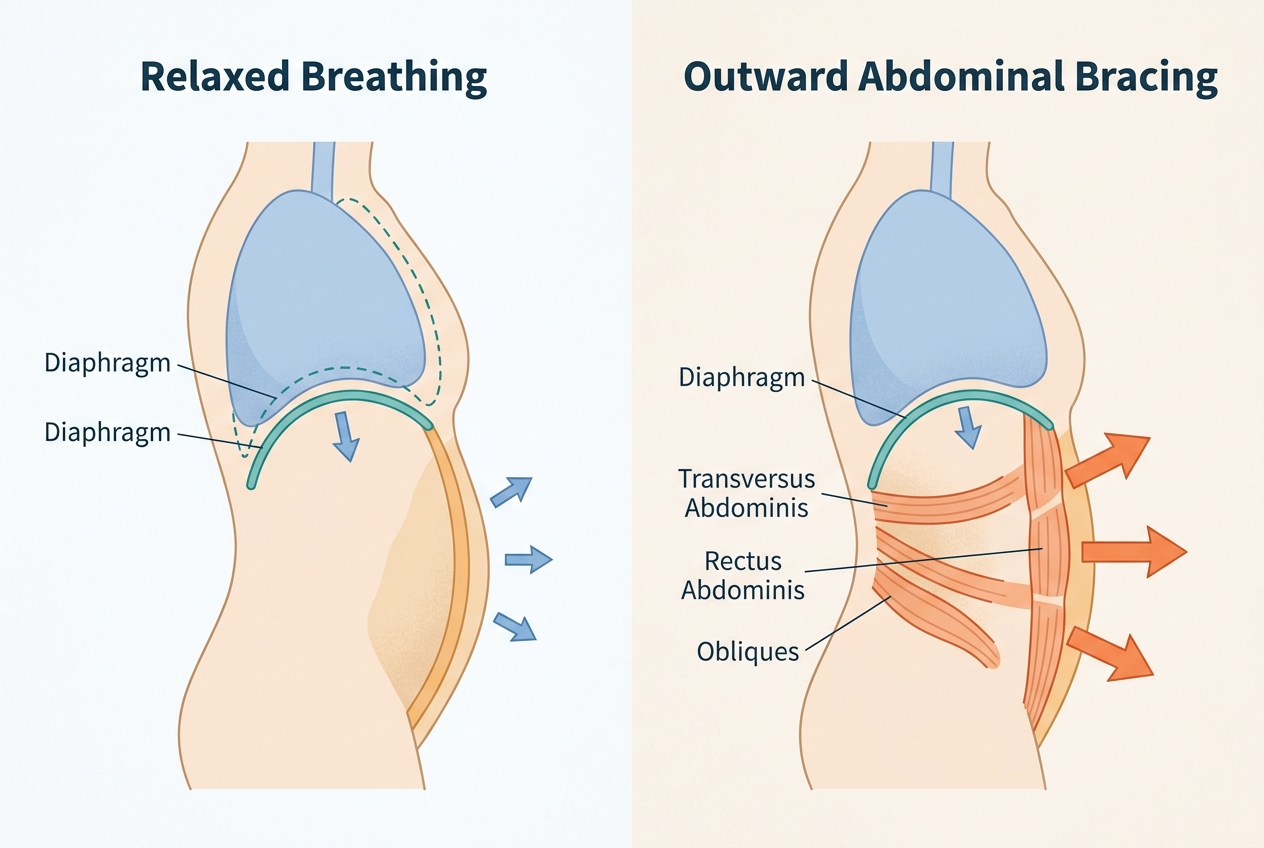
Forcing the abdomen outward can make visible distension look worse because the abdominal wall controls how abdominal contents are held, even when gas volume is not dramatically elevated. A 2023 narrative review in Clinical and Translational Gastroenterology describes abdominophrenic dyssynergia as a pattern in which the diaphragm contracts downward while the anterior abdominal wall relaxes. That movement can push the abdomen outward and create visible distension. This does not prove that every person with bloating is “just using their abs wrong.” It means the abdominal wall, diaphragm, gut sensation, and nervous system can interact. A useful first step is observation: note whether distension changes with posture, bracing, diaphragmatic breathing, bowel movements, stress, clothing pressure, and meal timing. The pattern matters more than one mirror check, because visible abdominal shape changes naturally through the day.
What else can cause bloating when tests are negative?
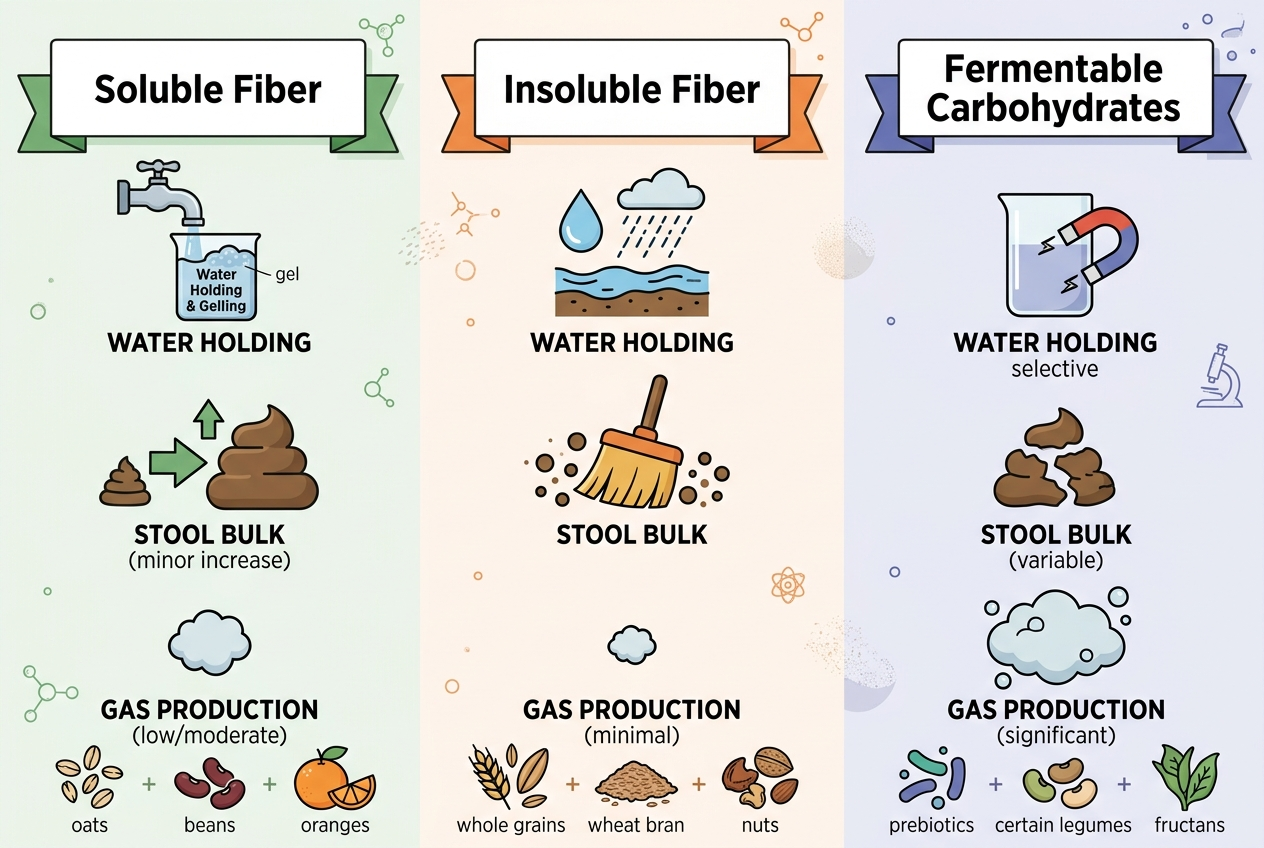
Negative tests reduce the chance of some conditions, but they do not erase functional digestive patterns. The NIDDK gas guide lists bloating, distension, belching, and flatulence as common gas-related symptoms, and it explains that swallowed air and bacterial fermentation can both contribute. Food triggers such as lactose, fructose, sorbitol, high-FODMAP foods, large fatty meals, carbonated drinks, and rapid eating can affect gas production or gas handling. Constipation can make normal gas feel more uncomfortable because stool retention changes pressure and transit. Gut-brain interaction disorders can amplify sensation even when imaging or blood work looks reassuring. Pelvic floor dysfunction can also affect evacuation and pressure. Medication changes, menstrual timing, and stress can shift the same baseline pattern. A negative test result should shift attention toward patterns, not toward random supplement trials or repeated restriction diets.
How can breathing and posture be tested safely?
Breathing and posture can be tested safely with low-risk observation, not forceful abdominal training. Sit upright, place one hand on the chest and one hand over the lower ribs, and breathe slowly without pushing the belly outward on purpose. Diaphragmatic breathing should feel like gentle rib and abdominal expansion, not like straining. Mayo Clinic specialists describe chronic bloating and distension as involving gut-brain interaction, visceral sensitivity, pelvic floor dysfunction, and abnormal diaphragm-abdominal wall coordination in some patients. A 2024 randomized trial in Gastroenterology found that thoracoabdominal wall motion-guided biofeedback improved visible distension by correcting abdominophrenic dyssynergia, but that intervention used guided training rather than internet guessing. If symptoms improve with relaxed breathing, the finding is useful information to bring to a clinician, physiotherapist, or dietitian, especially when food changes have not explained the pattern.
What should someone track before changing their routine?
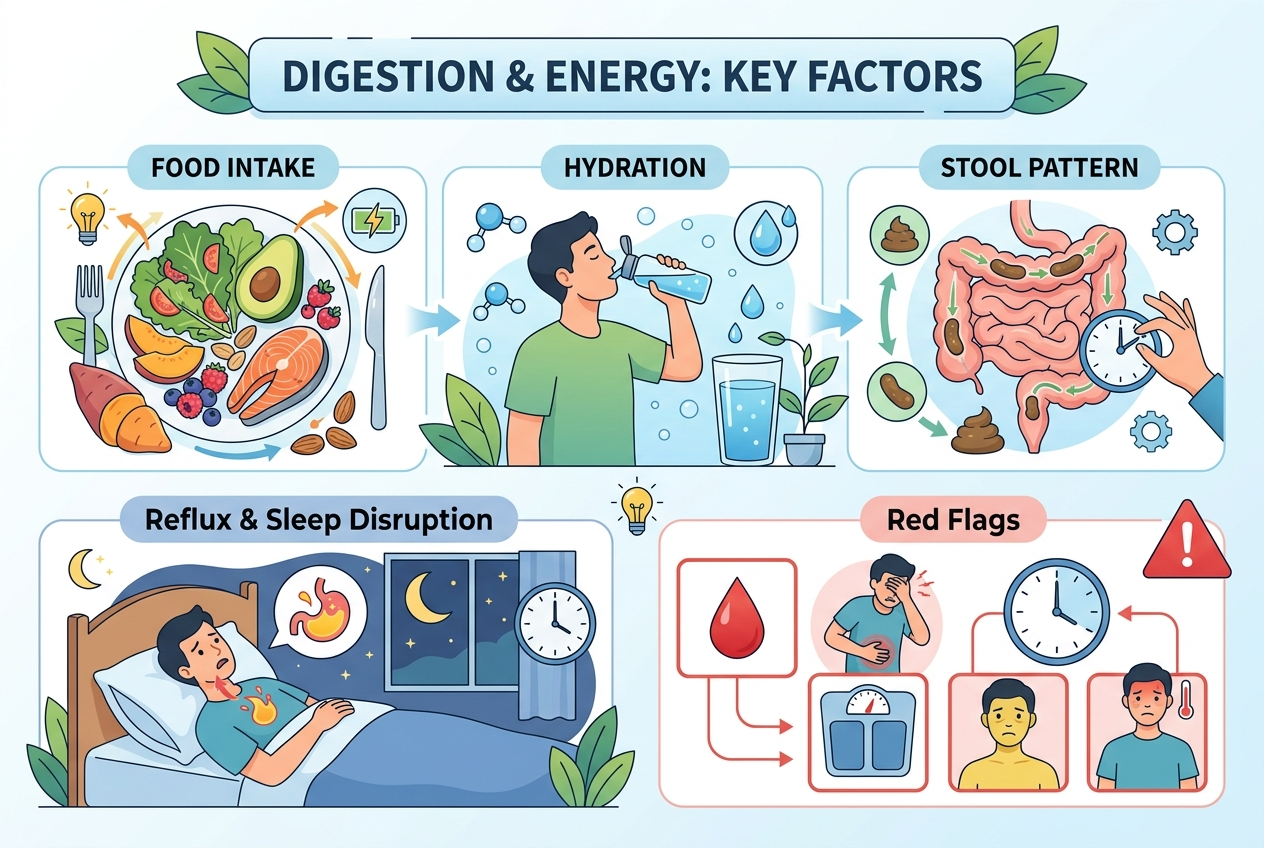
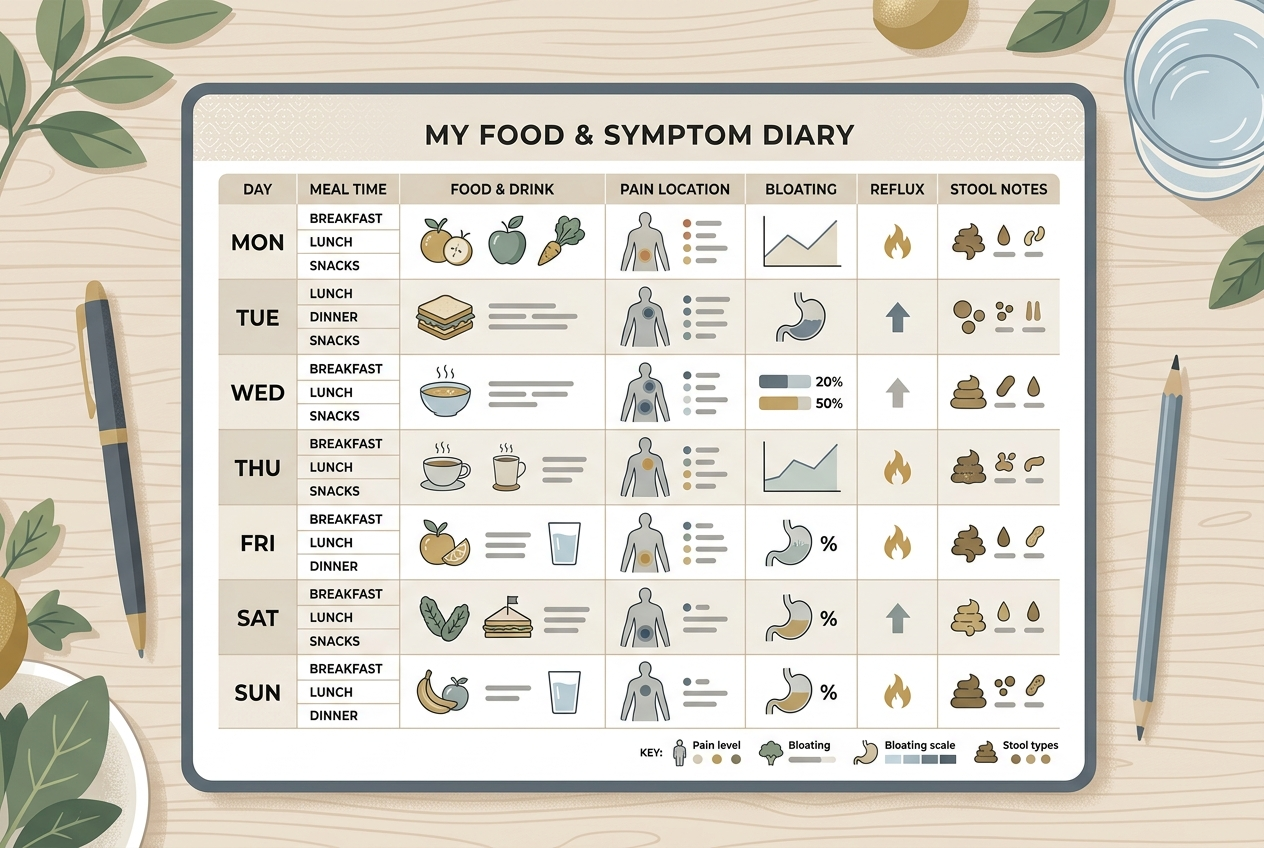
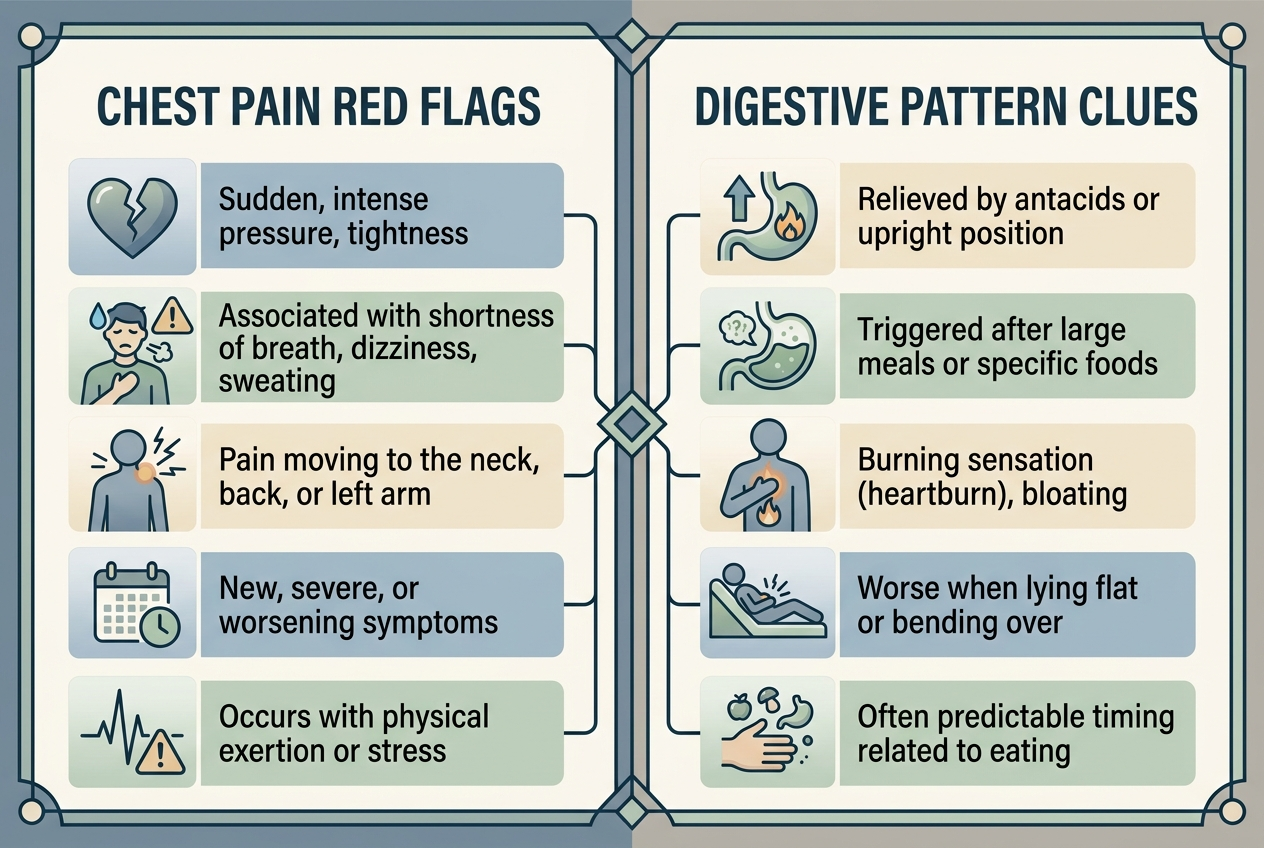
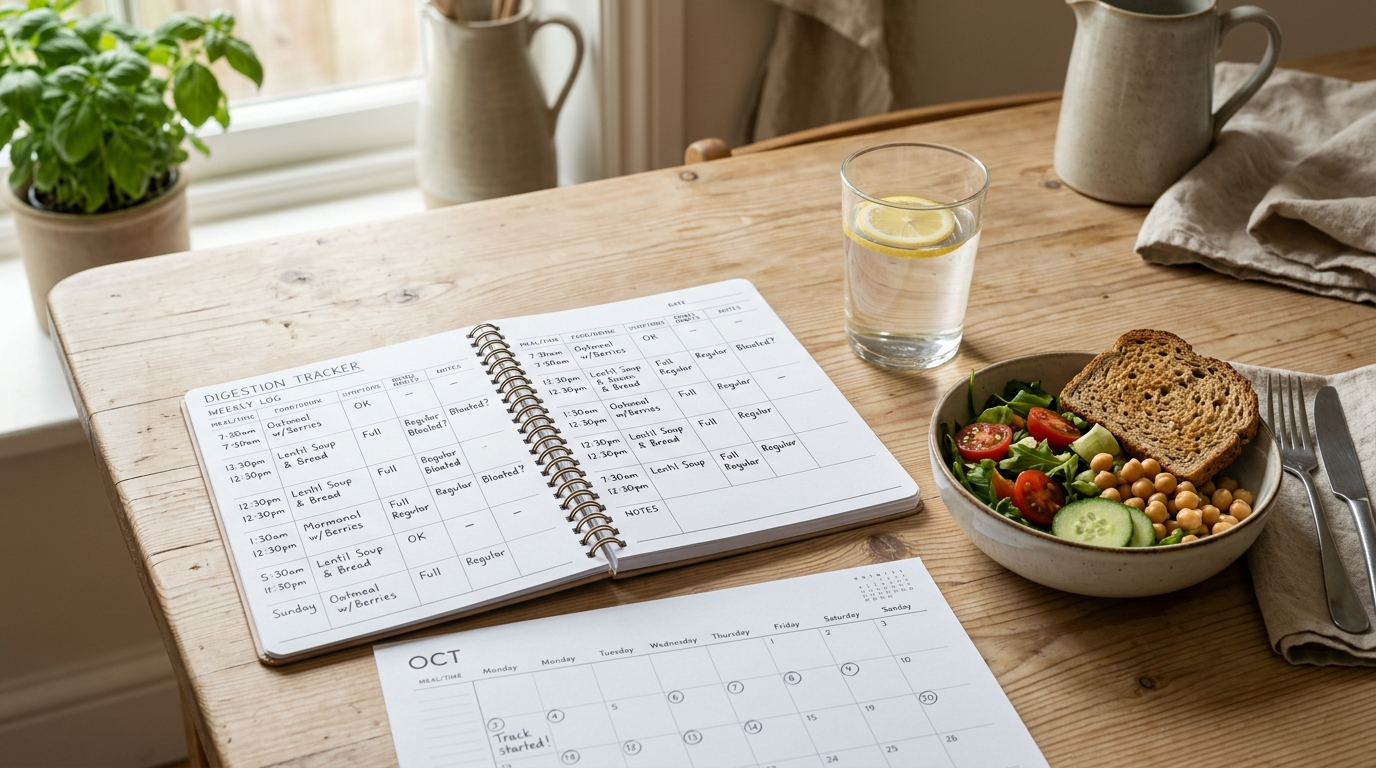
Track visible distension, abdominal pressure, meals, stool frequency, stool form, menstrual timing if relevant, stress, sleep, medications, carbonated drinks, gum chewing, and posture cues for two weeks. The goal is to identify repeatable relationships, not to prove one theory. A simple log can show whether distension appears after specific foods, after constipation, during stress, late in the day, or during abdominal bracing. Photos can help only if they are taken consistently, such as morning and evening in the same posture, without turning body checking into a new stress loop. Red flags deserve a different path: blood in stool, unexplained weight loss, fever, vomiting, anemia, new severe pain, persistent diarrhea, progressive swelling, or postmenopausal new bloating should be discussed with a clinician. Pattern tracking is useful because it creates a cleaner conversation and reduces the temptation to change five variables at once.
What approaches are worth discussing with a professional?
The most useful professional options depend on the pattern. Best for posture-linked visible distension: referral to a clinician familiar with abdominophrenic dyssynergia, diaphragmatic breathing, or biofeedback. Best for constipation-linked bloating: stool pattern assessment, fiber tolerance review, hydration, activity, and pelvic floor screening. Best for food-triggered bloating: a registered dietitian-guided lactose, fructose, or low-FODMAP trial rather than permanent broad restriction. Best for stress-linked symptoms: gut-directed behavioral tools, sleep consistency, and nervous-system regulation. Best for persistent unexplained distension: follow-up medical review rather than assuming every prior test covered every possibility. A practical approach published in Clinical Gastroenterology and Hepatology notes that bloating and distension often require a targeted history across diet, constipation, pelvic floor function, and gut-brain disorders. The right next step is pattern-matched, not one-size-fits-all, and the first professional visit is easier when the log is specific.
What questions do people ask about negative-test bloating?
Is visible bloating always caused by gas?
No. Visible distension can involve gas, stool burden, fluid, posture, abdominal wall relaxation, diaphragm movement, or visceral sensitivity. Gas is common, but it is not the only explanation.
What is abdominophrenic dyssynergia?
Abdominophrenic dyssynergia is an abnormal coordination pattern between the diaphragm and abdominal wall. The diaphragm moves downward and the abdominal wall relaxes, which can push the abdomen outward.
Can bad posture cause bloating?
Posture can change how abdominal contents are held and how distension looks. It should be treated as one possible contributor, not a complete diagnosis.
Should I keep doing ab exercises if bracing worsens distension?
Do not force exercises that reliably worsen symptoms. Discuss the pattern with a clinician or physiotherapist who can assess breathing mechanics, pelvic floor function, and abdominal wall coordination.
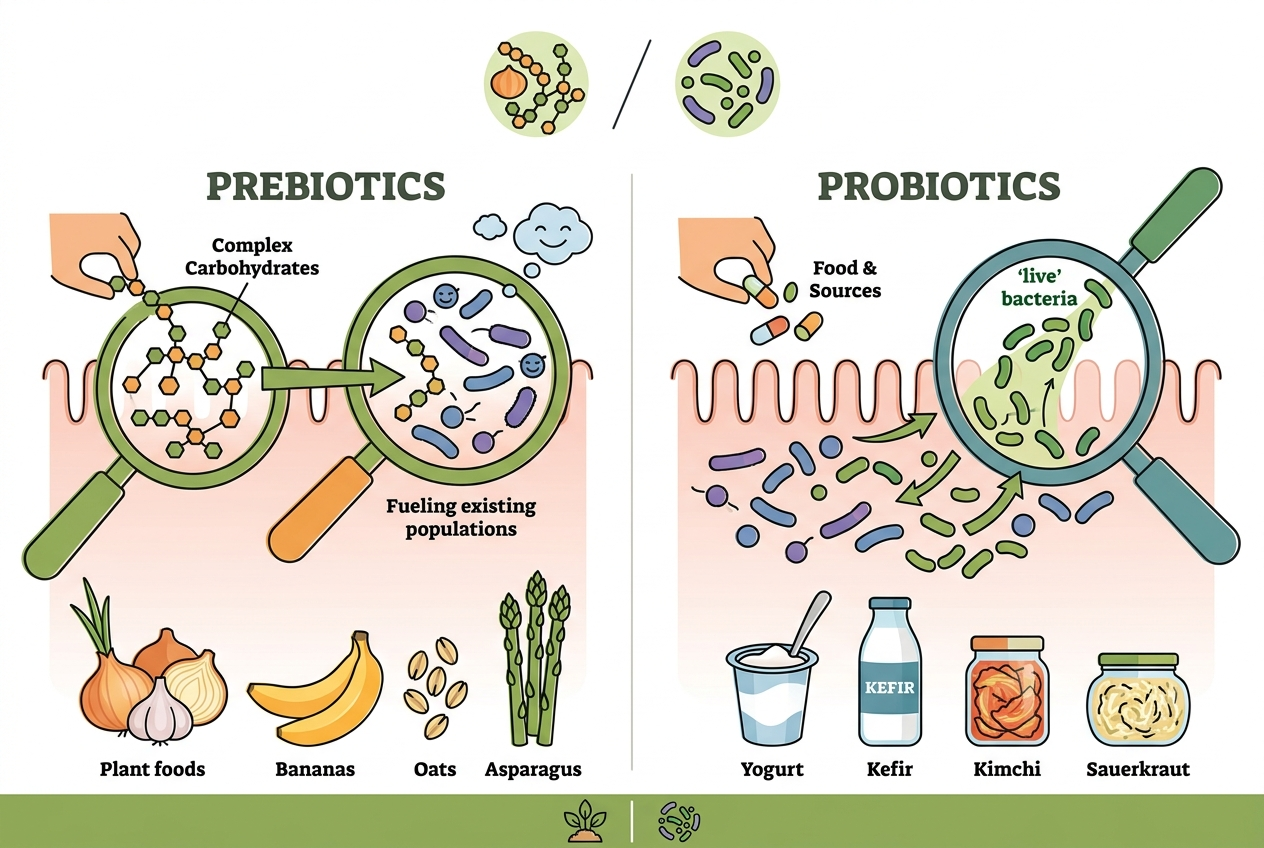
Can a low-FODMAP diet fix this?
A low-FODMAP trial can help some food-triggered bloating patterns, but it will not correct every posture-linked or pelvic-floor-linked pattern. It works best when guided by a dietitian and followed by reintroduction.
When is bloating with negative tests still concerning?
New, progressive, painful, or persistent bloating deserves review, especially with weight loss, blood, vomiting, fever, anemia, or postmenopausal onset. Negative past tests do not replace follow-up when symptoms change.
What is the safest first experiment?
The safest first experiment is a two-week symptom log plus gentle relaxed breathing practice. Avoid new restrictive diets, multiple supplements, or aggressive abdominal training until the pattern is clearer.
Negative-test bloating is real, even when standard testing does not show a single cause. Abdominal wall coordination, food tolerance, constipation, pelvic floor function, and gut-brain sensitivity can all matter, so the best next step is careful pattern tracking and targeted professional support.