
Bloating can get worse in your 40s even when diet looks unchanged because digestion, hormones, stool pattern, activity, medications, and food tolerance can change. The food may be the same, but gut motility, gas handling, constipation risk, and sensitivity to fermentable carbohydrates may not be the same.
How did we evaluate bloating changes in your 40s?
We evaluated age-related bloating by separating common physiology from red-flag symptoms. We prioritized NIDDK, Mayo Clinic, peer-reviewed microbiome reviews, and clinical nutrition references over anecdotal supplement claims or single-cause explanations. We excluded product recommendations because this is a cold-stage educational question and the user does not yet need a buying guide. We treated “diet has not changed” as a useful observation, not proof that digestion has stayed identical. We looked for repeatable patterns that a reader can track without restricting foods unnecessarily. We also separated symptom education from diagnosis because abdominal distension has many overlapping causes in clinical digestive practice today. The main limitation is that bloating can reflect constipation, lactose intolerance, FODMAP intake, perimenopause, stress physiology, medication effects, pelvic floor changes, or medical conditions, so persistent or severe symptoms need individualized medical evaluation.
Why can the same diet cause more bloating after 40?
The same diet can cause more bloating after 40 because the digestive context around the diet can change. The NIDDK explains that gas in the digestive tract can come from swallowed air and bacterial fermentation of carbohydrates. If stool moves more slowly, gas can feel more trapped even when meals look familiar. If activity drops, hydration changes, or fiber intake stays high without enough fluid, constipation-linked bloating can increase. If lactose tolerance changes, the same milk, yogurt, or whey-containing food can create more gas. If onions, garlic, wheat, beans, or certain sweeteners appear often, fermentable carbohydrates can exceed a new tolerance threshold. The important point is that “same diet” does not mean “same digestion.” The body processes the same inputs under different motility, hormone, stress, medication, sleep, and activity conditions. That context changes the result of familiar meals.
How do hormones affect bloating in your 40s?
Hormonal transition can affect bloating in the 40s because estrogen and progesterone influence fluid balance, bowel motility, and visceral sensitivity. Mayo Clinic notes that perimenopause can begin years before menopause and may include cycle changes, sleep disruption, and body changes (Mayo Clinic). Those shifts do not mean every bloating episode is hormonal, but they can change the background conditions around digestion. Progesterone can slow gastrointestinal movement for some people, and slower movement can make stool and gas feel more uncomfortable. Sleep disruption can also change meal timing, caffeine use, stress reactivity, and constipation risk. A useful pattern check compares bloating timing with menstrual cycle phase, sleep quality, bowel movements, and high-fermentation meals. Hormones can be part of the pattern without being the only cause, especially when symptoms cluster around predictable cycle windows. A cycle-aware log can make that pattern visible.
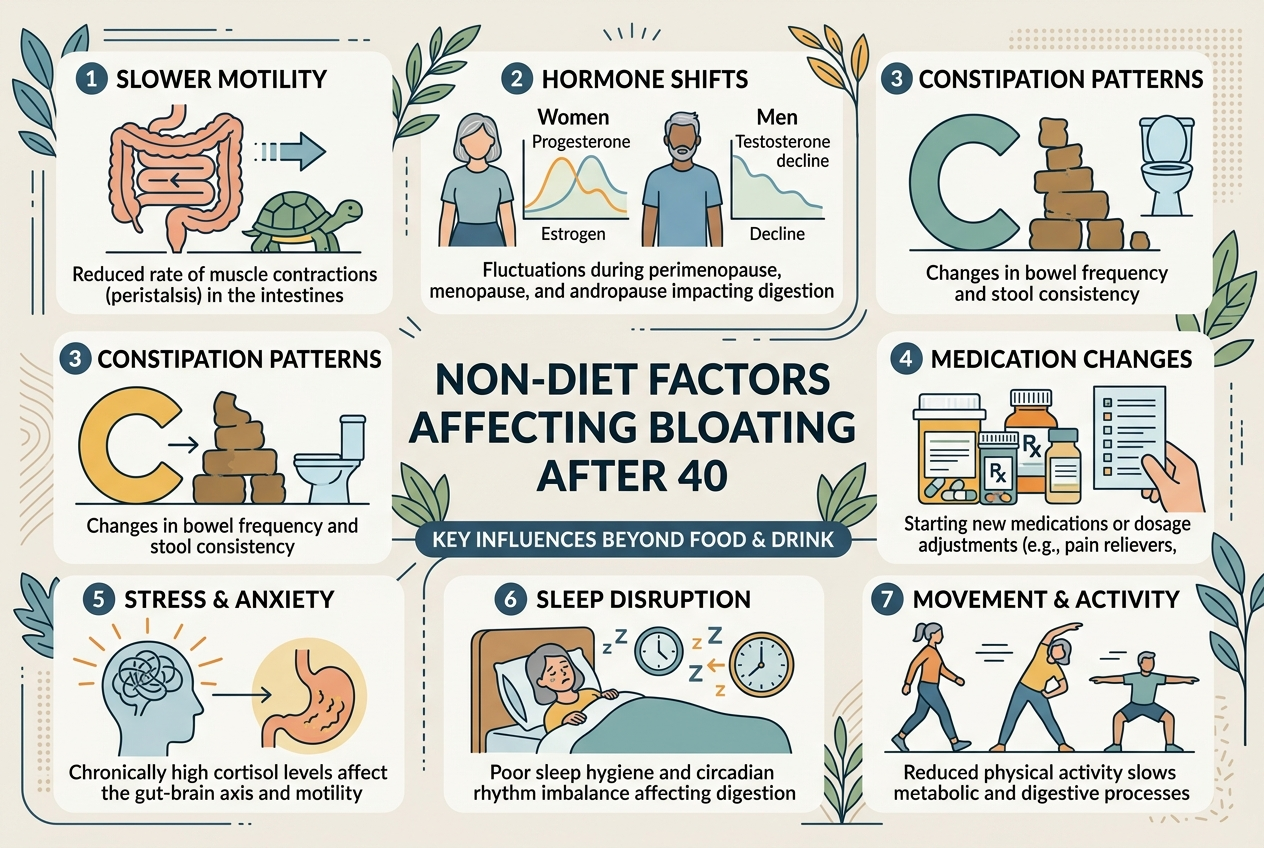
What non-diet factors commonly increase bloating?
Non-diet factors commonly increase bloating by changing motility, pressure, or gas perception. Reduced walking, strength training, or daily movement can slow bowel habits. New medications, including some acid reducers, iron, calcium, pain relievers, and antidepressants, can change constipation risk or upper-gut comfort. Stress can alter gut-brain signaling and make normal gas feel more intense. Eating speed can increase swallowed air. Carbonated drinks can add gas volume. Constipation can make the abdomen feel tight even when calories and food choices are unchanged. Pelvic floor coordination can also affect evacuation, which changes pressure after meals. A practical review should list the last three months of medication changes, sleep changes, exercise changes, travel, stress spikes, bowel frequency, and meal timing. That list often explains why a familiar diet suddenly feels unfamiliar after meals. The pattern may be behavioral, not dietary.
When should bloating in your 40s be checked?
Bloating in your 40s should be checked when it is new, persistent, severe, worsening, or paired with warning signs. The NIDDK lists symptoms such as blood in stool, vomiting, diarrhea, constipation, unexplained weight loss, and persistent abdominal pain as reasons to seek care for gas-related concerns (NIDDK). Sudden appetite loss, fever, anemia, black stools, repeated vomiting, trouble swallowing, or pain that wakes someone at night also deserves medical attention. Most bloating is not an emergency, but age should lower the threshold for a careful review when symptoms change without an obvious reason. A clinician can decide whether constipation care, food intolerance testing, medication review, pelvic floor evaluation, imaging, bloodwork, or endoscopy is appropriate. Self-tracking helps, but red flags need diagnosis, not guessing or online reassurance. Timely review protects against missed causes and delayed evaluation.
What can you track before changing your diet?
Track bowel pattern, meal timing, and symptom timing before changing the whole diet. Record stool frequency, stool form, bloating severity, gas, abdominal pressure, menstrual cycle phase, sleep, movement, and medication timing for two weeks. Note high-fermentation meals that contain beans, onions, garlic, wheat, apples, stone fruit, dairy, sugar alcohols, or carbonated drinks. The goal is not to create a perfect food diary; the goal is to spot repeated triggers. If bloating is worse on low-movement days, motility may matter. If bloating is worse around certain cycle phases, hormones may matter. If bloating is worse after dairy, lactose may matter. If bloating is worse when stool frequency drops, constipation may matter. A clean log prevents unnecessary restriction and gives a clinician better information than memory alone. It also makes small experiments safer and more specific.
What questions do people ask about bloating after 40?
Can bloating increase during perimenopause?
Yes, bloating can increase during perimenopause for some people. Hormonal shifts can interact with fluid balance, constipation tendency, sleep, and gut sensitivity.
Can constipation cause a pregnant-looking belly?
Yes, constipation can create abdominal pressure, trapped gas, and visible distension. Persistent or painful distension should be checked, especially when it is new.
Can lactose intolerance appear later in life?
Yes, lactose tolerance can change over time. A two-week dairy pattern check can help identify whether milk, ice cream, whey, or soft cheeses repeatedly match symptoms.
Should I cut out all high-FODMAP foods?
Not without a plan. Broad restriction can reduce diet quality, so a clinician or dietitian-guided approach is better for persistent symptoms.
Are probiotics the first step for bloating after 40?
Not always. Stool pattern, food triggers, medications, activity, and red flags should be reviewed before assuming a probiotic is the right first move.
When is bloating urgent?
Bloating is more urgent when it comes with severe pain, vomiting, blood in stool, black stools, fever, unexplained weight loss, anemia, or progressive worsening. Those symptoms need medical care.
What is the practical next step?
Start with a two-week pattern log instead of changing everything at once. Track stool frequency, bloating timing, cycle phase, activity, sleep, medications, dairy, carbonated drinks, and high-fermentation foods. If the log points to constipation, lactose, eating speed, or low movement, address that pattern first. If symptoms are severe, persistent, new, or paired with red flags, book a medical evaluation. The useful answer is usually not that the diet secretly changed; it is that the digestive context around the diet changed. That framing helps narrow the next step without turning a familiar diet into an unnecessary restriction project. Bring the log to a clinician if symptoms persist. It can shorten the conversation, reduce guesswork, and show whether the problem is stool pattern, food tolerance, medication timing, cycle timing, or something that needs testing soon safely.
Leave a Reply