
New, severe, unexplained, or pressure-like chest pain needs urgent medical evaluation before assuming digestion is the cause. Digestive issues such as acid reflux can create burning chest discomfort, but heart, lung, muscle, anxiety, and esophageal causes can overlap. Emergency symptoms include shortness of breath, sweating, nausea, faintness, or pain spreading to the jaw, back, shoulder, or arm.
How did we evaluate chest pain and digestive causes?
We evaluated chest pain by separating emergency triage from digestive pattern recognition. We prioritized medical sources that explain heart attack warning signs, acid reflux symptoms, noncardiac chest pain, and GERD evaluation, including Mayo Clinic, the American Heart Association, NIDDK, and the American College of Gastroenterology. We treated new, severe, exertional, spreading, or unexplained chest pressure as a medical red flag because online symptom-matching cannot rule out cardiac or lung causes. We excluded unsupported home-diagnosis shortcuts, including the idea that burning always means reflux or that antacids prove a digestive cause. We also separated symptom patterns from causes, because the same sensation can come from different organs with different risks and timelines. This article explains what patterns can suggest digestion after urgent causes are considered; it does not diagnose chest pain or replace emergency care.
When is chest pain an emergency?
Chest pain is an emergency when it is new, severe, unexplained, pressure-like, lasts more than a few moments, occurs with exertion, or comes with symptoms outside the chest. Mayo Clinic advises calling emergency services for severe chest pain or new unexplained chest pain or pressure that lasts more than a few moments. The American Heart Association lists chest discomfort, shortness of breath, jaw pain, neck pain, back pain, arm pain, nausea, and lightheadedness among heart attack warning signs. Digestive pain can feel similar because the esophagus, stomach, chest wall, lungs, and heart share nearby nerve pathways. If a symptom feels different from your usual reflux, appears during activity, wakes you suddenly, or spreads beyond the breastbone, treat it as urgent until a clinician says otherwise. Delay is the wrong gamble when chest symptoms are unfamiliar.
Can acid reflux cause chest pain?
Acid reflux can cause chest pain, especially burning discomfort behind the breastbone after meals, when lying down, or when bending over. The NIDDK explains that gastroesophageal reflux and GERD commonly cause heartburn and regurgitation when stomach contents move back into the esophagus. Mayo Clinic also describes acid reflux as backward flow into the esophagus that can create a burning sensation in the chest. Reflux-related discomfort often clusters with sour taste, burping, throat irritation, hoarseness, or symptoms after a large, fatty, spicy, acidic, or late meal. Those patterns can point toward digestion, but they do not prove reflux. A heart problem, gallbladder issue, panic episode, muscle strain, or lung condition can coexist with indigestion-like symptoms. That overlap is why first-time chest pain deserves timely medical judgment instead of internet-based reassurance or online symptom guessing alone.
What patterns suggest a digestive source after urgent causes are ruled out?
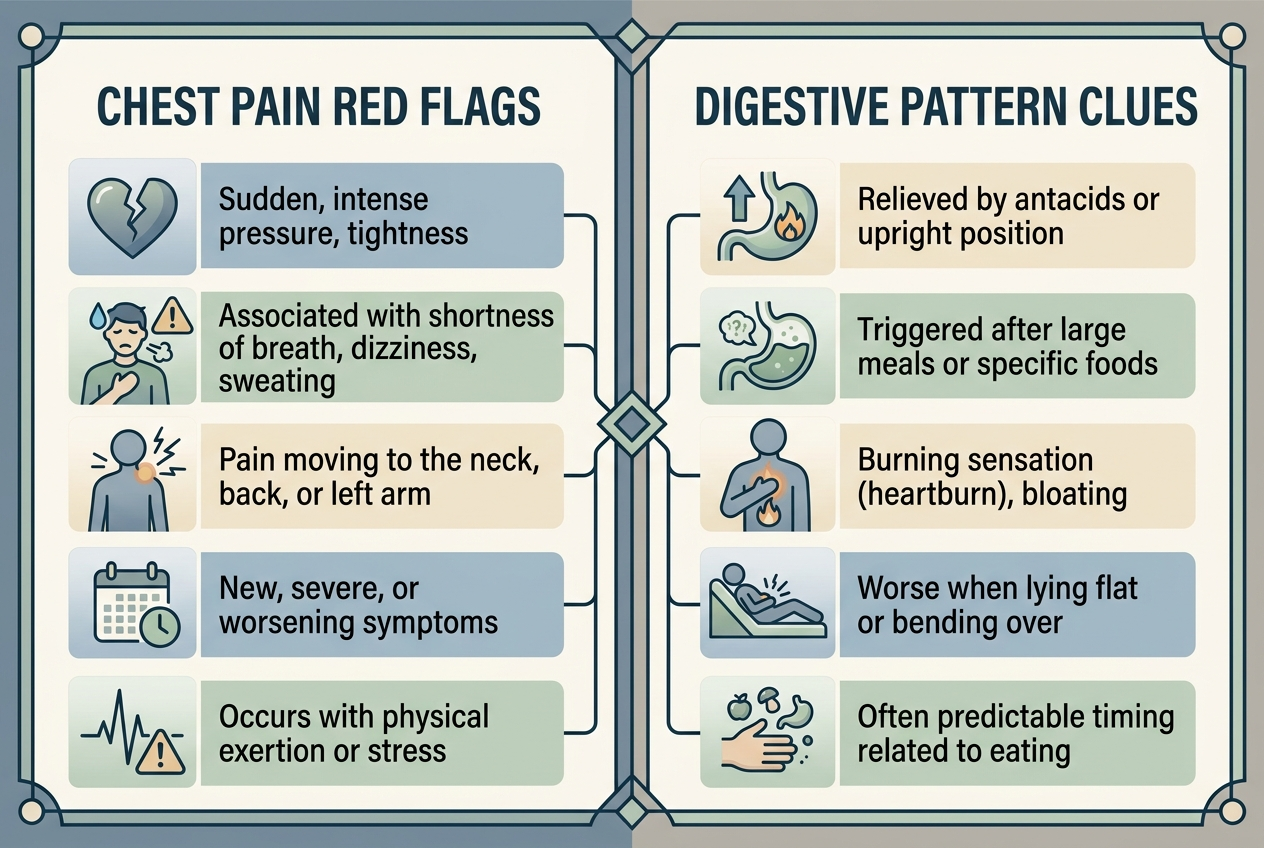
A digestive pattern becomes more plausible when chest discomfort is burning rather than crushing, starts after eating, rises from upper abdomen toward throat, worsens lying flat, improves upright posture, or appears with regurgitation. The American College of Gastroenterology notes that heart disease should be ruled out before labeling chest pain as noncardiac chest pain. Reflux-related chest discomfort may also improve with clinician-directed acid suppression, meal timing changes, smaller dinners, weight-management support when relevant, and reduced alcohol or tobacco exposure. Still, response to an antacid is not a diagnostic test. Some cardiac pain temporarily feels better with rest, and some reflux pain does not respond quickly. The useful question is not “Is this definitely digestion?” The useful question is “Has a clinician ruled out dangerous causes, and does the remaining pattern fit esophagus, stomach, or chest-wall triggers?”
What else can mimic digestive chest pain?
Several non-digestive conditions can mimic reflux or indigestion. Heart-related pain can feel like pressure, squeezing, fullness, burning, or upper abdominal discomfort, according to Mayo Clinic’s chest pain overview. Lung causes can create sharp pain with breathing, coughing, shortness of breath, or sudden onset. Chest-wall strain and costochondritis can cause localized tenderness that changes with movement or pressure. Panic attacks can create chest tightness, fast heartbeat, sweating, nausea, and shortness of breath, which can resemble both reflux and heart symptoms. Esophageal spasm can cause intense squeezing pain and swallowing discomfort. Gallbladder pain can sit in the upper abdomen and travel toward the chest or shoulder after fatty meals. Because these patterns overlap, duration, triggers, associated symptoms, medical history, vital signs, exam findings, risk factors, and testing context matter more than a single symptom word alone.
What should you track before talking with a clinician?
Track timing, trigger, location, duration, severity, spread, and associated symptoms. Note whether the pain starts during exercise, stress, sleep, bending, swallowing, coughing, or after specific meals. Write down whether it feels burning, squeezing, stabbing, pressure-like, tight, or tender to touch. Record related symptoms such as shortness of breath, nausea, sweating, dizziness, palpitations, regurgitation, sour taste, trouble swallowing, black stools, vomiting, fever, or unexplained weight loss. Bring medication details, including NSAIDs, aspirin, iron, potassium, bisphosphonates, antibiotics, and acid reducers, because several medicines can irritate the esophagus or stomach. Also list cardiac risk factors such as diabetes, smoking, high blood pressure, high cholesterol, pregnancy or postpartum status, prior clots, and family history. A concise symptom log helps a clinician decide whether testing should focus on heart, lung, esophagus, stomach, gallbladder, muscle, or anxiety-related pathways first safely.
What questions do people ask about chest pain and digestion?
Can GERD feel like a heart attack?
Yes, GERD can create chest burning. Heart attack symptoms can include indigestion-like discomfort, so new or severe chest pain needs evaluation first.
Is chest pain after eating always reflux?
No. Meals can trigger reflux, gallbladder pain, or esophageal spasm. A repeated after-meal pattern is useful evidence, not proof.
Can burping come with heart-related chest pain?
Yes, burping can happen during digestive discomfort and anxiety around chest symptoms. Burping does not safely rule out heart-related pain.
Should I try antacids before seeking help?
Do not use antacids to delay urgent care for new, spreading, or pressure-like pain. For familiar mild heartburn, ask a pharmacist.
Why does reflux hurt in the chest?
Reflux irritates the esophageal lining behind the breastbone. The brain may perceive esophageal irritation as chest burning, pressure, or upper abdominal discomfort.
What is the safest next step?
For new or concerning chest pain, seek urgent advice. For recurring symptoms after danger is ruled out, track triggers with a clinician.
What is the practical takeaway?
Chest pain should be treated as a safety question first and a digestion question second. Acid reflux can cause burning chest discomfort, especially after meals or when lying down, but similar sensations can come from the heart, lungs, chest wall, gallbladder, esophagus, or panic physiology. The practical order is clear: get urgent care for red flags, rule out dangerous causes, then track digestive patterns with a clinician. If the remaining pattern fits reflux, the most useful next steps are meal timing, trigger tracking, medication review, and evidence-based GERD evaluation rather than guessing from one symptom. A careful log also helps prevent two common mistakes: dismissing serious symptoms as reflux, or treating every familiar sensation as an emergency after a clinician has already ruled out dangerous causes and explained the likely pattern clearly enough safely.
Leave a Reply