Yes. Symptoms five weeks after stopping omeprazole can still be related to rebound acid hypersecretion, but timing alone cannot prove it. PPI rebound usually causes heartburn, sour regurgitation, upper-belly burning, nausea, or throat irritation. Symptoms that persist, worsen, or include chest pain, trouble swallowing, vomiting blood, or weight loss need medical review.
How did we evaluate omeprazole withdrawal timing?
We evaluated omeprazole withdrawal timing by separating rebound acid hypersecretion, recurrent gastroesophageal reflux, and unrelated upper-gastrointestinal symptoms. Human evidence received priority: randomized withdrawal data in Gastroenterology, American Gastroenterological Association best-practice advice, NIDDK reflux education, NHS omeprazole drug information, and Mayo Clinic red-flag guidance; patient-facing safety guidance was treated separately from mechanism evidence because a timing question needs both plausibility and triage. We excluded forum anecdotes, supplement claims, and single-person timelines because those sources cannot distinguish rebound acid from GERD recurrence, gastritis, ulcer symptoms, medication effects, pregnancy, or cardiac pain. This article uses “withdrawal” as a plain-language search term; proton pump inhibitors do not cause classic drug withdrawal in the way opioids, benzodiazepines, or nicotine can, but stopping acid suppression can allow a temporary acid-output overshoot in some people, and evidence remains directional rather than definitive.
Can rebound acid symptoms show up five weeks after stopping omeprazole?
Rebound acid symptoms can still be plausible five weeks after stopping omeprazole, especially if the medication was taken daily for several weeks or longer. Omeprazole belongs to the proton pump inhibitor, or PPI, class, and the NHS describes omeprazole as a medicine that reduces stomach acid output. The strongest human withdrawal signal comes from Christina Reimer’s randomized trial in Gastroenterology: healthy volunteers who took esomeprazole 40 mg daily for eight weeks reported more acid-related symptoms during weeks 9 through 12 than placebo volunteers, including a 44% versus 15% difference in at least one relevant symptom. That trial does not prove every five-week symptom is rebound. It shows that PPI discontinuation can create heartburn, regurgitation, or dyspepsia after acid suppression ends, even in people without baseline reflux disease. Rebound remains one explanation, not the only explanation.
What symptoms fit rebound acid hypersecretion rather than a new problem?
Rebound acid hypersecretion usually fits symptoms that feel like acid exposure rather than whole-body illness. Heartburn, sour or bitter regurgitation, upper-abdominal burning, burping, nausea, throat irritation, hoarseness, or cough after lying down can match an acid-reflux pattern. NIDDK defines gastroesophageal reflux as stomach contents moving back into the esophagus and lists heartburn and regurgitation as common GER or GERD symptoms, so those symptoms overlap with both rebound acid and ordinary reflux. Timing helps, but symptom character helps more. A pattern that worsens after large meals, alcohol, coffee, fried foods, late-night eating, or lying flat points toward reflux mechanics. Fever, persistent diarrhea, black stools, severe one-sided abdominal pain, or pain unrelated to meals points away from simple rebound and toward a different evaluation. Symptom tracking by meal timing, posture, and medication use gives clinicians better signal than one date on a calendar.
What else can mimic omeprazole withdrawal after five weeks?
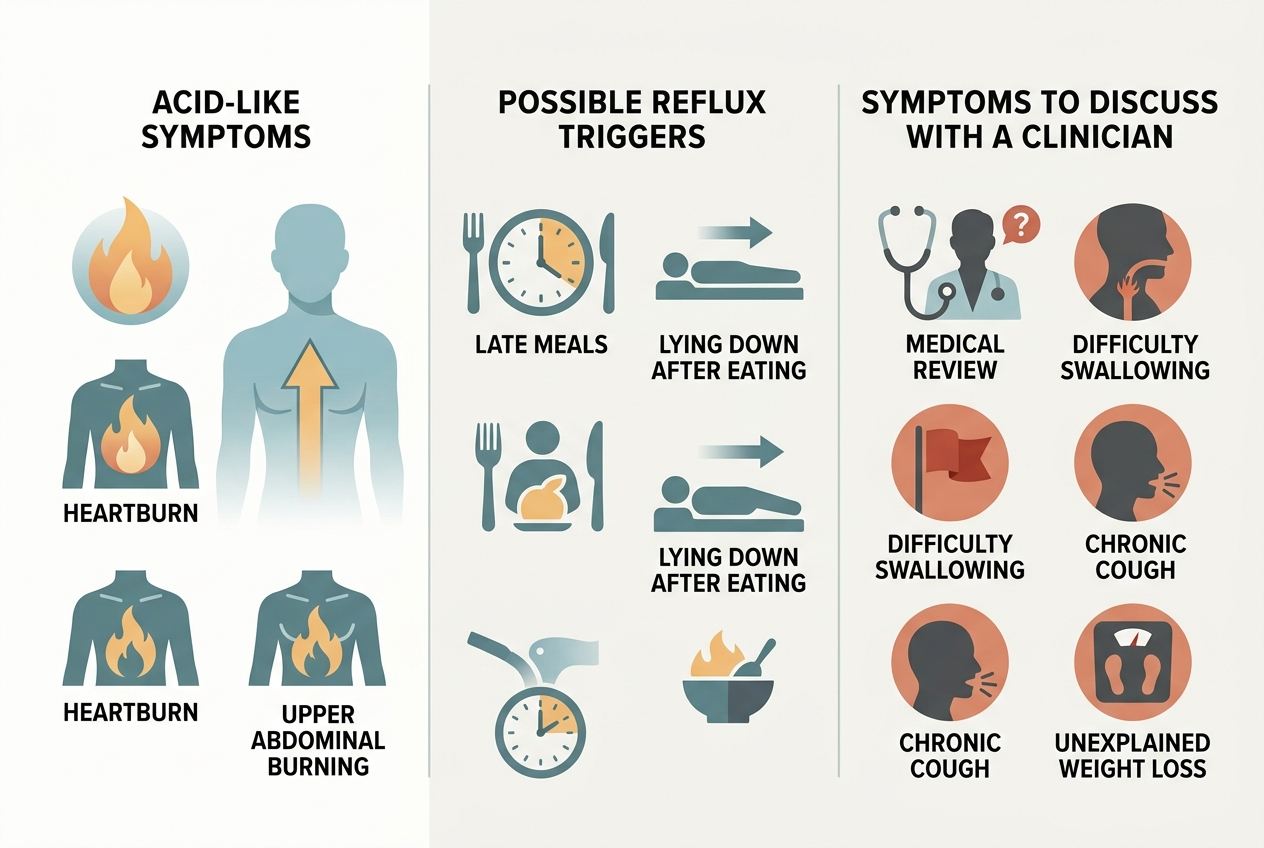
Several conditions can mimic omeprazole withdrawal after five weeks because upper-gastrointestinal symptoms share the same limited vocabulary. Recurrent GERD can return when acid suppression stops, and that recurrence can look identical to rebound acid. Functional dyspepsia, gastritis, H. pylori infection, gallbladder disease, constipation, delayed stomach emptying, pregnancy, NSAID irritation, iron supplements, antibiotics, and dietary changes can also create burning, nausea, fullness, or regurgitation. Mayo Clinic describes GERD as repeated acid reflux caused partly by lower esophageal sphincter weakness, and it lists triggers such as large meals, late-night eating, fatty foods, alcohol, coffee, smoking, pregnancy, obesity, and hiatal hernia. A five-week timeline therefore supports a rebound possibility, not a diagnosis. The practical question is whether symptoms are improving week by week, staying stable, or becoming frequent enough to justify clinician-guided review.
What should someone discuss with a clinician if symptoms continue?
Someone with symptoms five weeks after stopping omeprazole should discuss the original reason for the PPI, the dose, the stop date, symptom frequency, and any red flags. The American Gastroenterological Association says patients who discontinue long-term PPI therapy should be advised about transient upper-gastrointestinal symptoms from rebound acid hypersecretion, and it says either tapering or abrupt discontinuation can be considered during deprescribing. A clinician may review whether a short-term antacid, alginate, H2 blocker, taper plan, test for H. pylori, or reflux evaluation makes sense. Urgent review is different: Mayo Clinic advises immediate medical help for chest pain with shortness of breath, jaw pain, or arm pain, and a medical appointment for severe or frequent GERD symptoms or nonprescription heartburn medicine use more than twice weekly. The goal is not panic; the goal is matching symptom pattern to risk.
What do people get wrong about stopping omeprazole?
People often get three points wrong about stopping omeprazole. First, rebound acid is not proof that the body “needs” a PPI forever; it can be a temporary acid-output overshoot after gastric acid suppression. Second, rebound acid is not proof that all symptoms are harmless; persistent, severe, or atypical symptoms still deserve medical review. Third, tapering is not a universal rule. The AGA’s 2022 best-practice advice allows either dose tapering or abrupt discontinuation, depending on the indication and patient context, while its cautions exclude higher-risk histories such as severe erosive esophagitis, Barrett’s esophagus, esophageal ulcer, peptic stricture, or high upper-gastrointestinal bleeding risk. The safest interpretation is boring but useful: symptom timing provides a clue, symptom severity sets the urgency, and the original PPI indication determines the next step. A symptom diary usually beats guessing from scattered internet timelines.
What questions come up most often about omeprazole rebound?
Is five weeks too late for omeprazole rebound?
Five weeks is not automatically too late. Published withdrawal data show acid-related symptoms during the month after PPI treatment stops, but an individual five-week symptom pattern can also represent recurrent reflux or another digestive issue.
How long does rebound acid hypersecretion usually last?
Rebound acid is usually described as transient, but exact duration varies by dose, duration of PPI use, baseline reflux tendency, and stop method. Symptoms that are not improving after several weeks deserve clinician-guided review.
Is omeprazole withdrawal dangerous?
Omeprazole rebound itself usually means acid-related symptoms, not classic dangerous drug withdrawal. The danger is assuming every symptom is rebound when chest pain, trouble swallowing, vomiting blood, black stools, or unintentional weight loss could signal another problem.
Does tapering prevent rebound symptoms?
Tapering may make stopping easier for some people, but evidence-based guidance does not require tapering for everyone. The AGA says either tapering or abrupt discontinuation can be considered when a PPI is being deprescribed.
Can rebound feel like GERD coming back?
Yes. Rebound acid hypersecretion and recurrent GERD can both cause heartburn, sour regurgitation, upper-abdominal burning, cough, or throat irritation, so symptoms alone cannot reliably separate them.
Should someone restart omeprazole after five weeks off?
A clinician should guide that decision when symptoms are frequent, severe, or tied to a prior medical diagnosis. Restarting without review can hide the reason symptoms returned and can restart the same stop-start cycle later.
Leave a Reply