
Fiber is necessary for digestive health, but tolerability depends on fiber type, dose, hydration, and gut sensitivity. Soluble fibers such as psyllium often feel different from coarse wheat bran or high-FODMAP foods. If fiber worsens gas or bloating, the better move is usually changing type and pace, not abandoning fiber entirely.
How we evaluated fiber necessity and tolerability?
We evaluated fiber by separating general nutrition guidance from digestive-symptom tolerance. Human trials, reviews, Monash University FODMAP resources, and NIH-hosted fiber summaries carried more weight than social media rules about “more fiber.” We excluded supplement-brand claims and rapid detox framing because this article is educational. The evidence supports fiber as a core dietary pattern, but tolerance varies by soluble versus insoluble fiber, fermentability, serving size, and underlying digestive conditions.
Why can fiber help digestion but still feel uncomfortable?
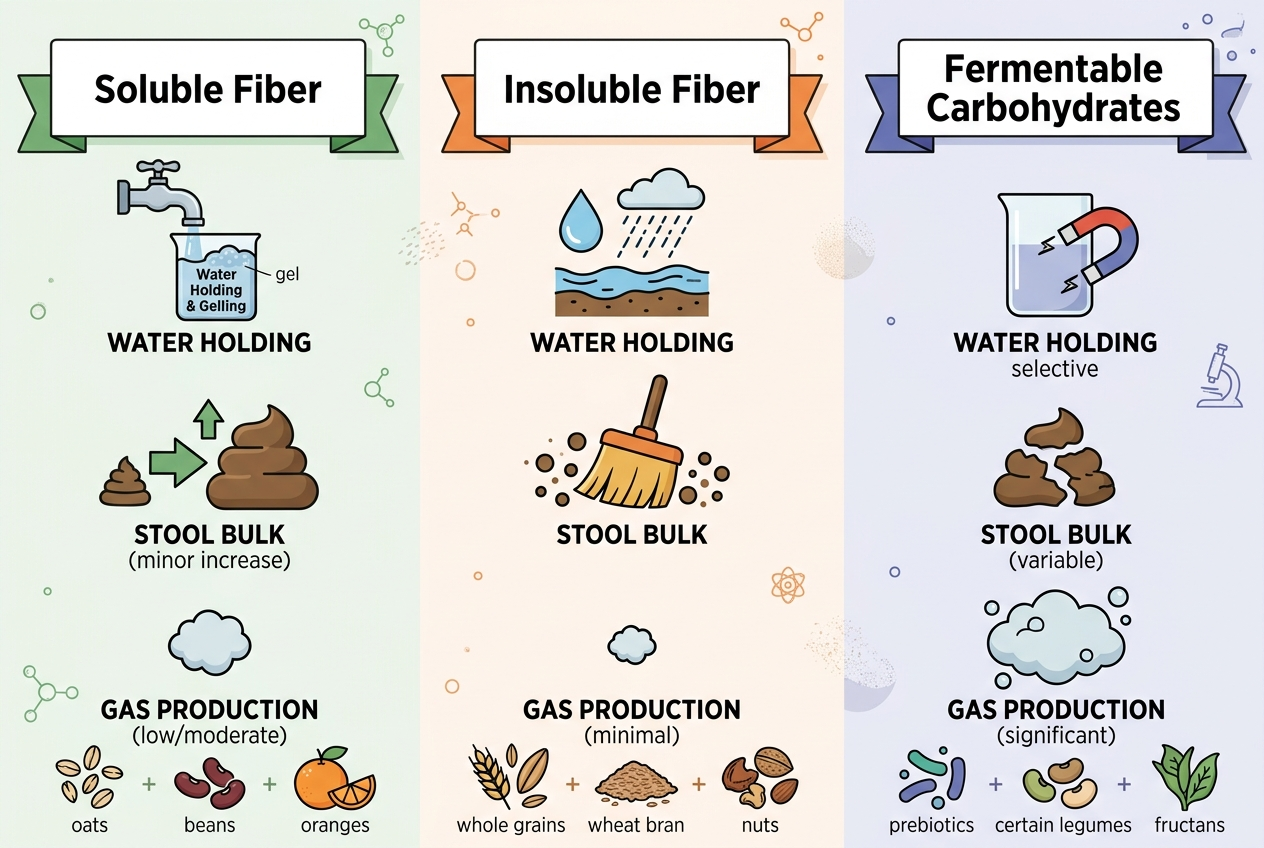
Fiber can help digestion because it changes stool bulk, water retention, transit time, and microbial fermentation. The same mechanisms can also create gas, pressure, or looser stool when the dose rises quickly. Soluble fibers such as psyllium form gels and are often easier to titrate, while coarse insoluble fibers such as wheat bran can feel harsher for some sensitive guts. A review on dietary fiber in irritable bowel syndrome reports that fiber supplementation, especially psyllium, can improve global IBS symptoms, while older primary-care research found soluble fiber performed better than bran. The practical lesson is specific: “eat more fiber” is incomplete advice. The useful question is which fiber, how much, how fast, and with how much fluid.
- Soluble fiber holds water and changes stool texture.
- Fermentable fiber feeds microbes and may increase gas during adaptation.
- Abrupt fiber increases are more likely to feel uncomfortable.
Which types of fiber are usually easier to tolerate?
Easier-tolerated fibers are often soluble, gel-forming, and introduced gradually. Psyllium, oats, chia, kiwi, and some partially hydrolyzed fibers tend to be discussed as gentler options because they can support stool form without the same rough texture as bran. Highly fermentable fibers, large bean servings, onions, wheat-heavy meals, and some sweeteners can create more gas in people with FODMAP sensitivity. Monash University explains that FODMAPs are short-chain carbohydrates that can draw water into the gut and ferment, contributing to bloating, gas, and pain in IBS. That does not make high-FODMAP foods “bad.” It means the same high-fiber food can be helpful for one person and poorly tolerated by another, especially during a flare or sudden diet change. Cooking method, portion size, and meal timing also change tolerance, so raw vegetables and cooked vegetables may not feel identical.
How should you increase fiber without making bloating worse?
Increase fiber slowly, with water, and with one change at a time. A practical starting point is adding a small serving of one fiber-rich food or one low-dose fiber source for several days before increasing again. The NIH notes that fiber benefits vary by fiber type, which means a single high-dose blend can be harder to interpret than a steady food-based change. If bloating rises sharply, reduce the dose rather than adding another digestive intervention. Timing also matters: spreading fiber across meals can feel easier than compressing it into one large serving. People who already have constipation, diarrhea, reflux, IBS, or recent gut infection should track stool pattern, gas, pain, and hydration while adjusting fiber. A gradual plan also protects confidence, because one rough day should not define the whole category. Keep meals otherwise familiar during the test window.
When is fiber not the whole answer?
Fiber is not the whole answer when symptoms are severe, new, persistent, or paired with red flags. Blood in stool, unintentional weight loss, fever, repeated vomiting, nighttime diarrhea, anemia, or escalating pain needs medical evaluation. Fiber also may not solve bloating that comes from lactose intolerance, celiac disease, medication changes, pelvic-floor dysfunction, small intestinal bacterial overgrowth, or high stress. Johns Hopkins Medicine notes that a low-FODMAP approach is often used with clinician or dietitian guidance for IBS and SIBO patterns, which shows why food triggers can matter as much as total fiber grams. Fiber remains important, but the right plan may involve food pattern testing, hydration, meal spacing, and medical context instead of simply chasing a larger number. If symptoms began suddenly, the timeline matters as much as the nutrition target. If symptoms improve and then return, dose timing and trigger stacking deserve another look.
What is a practical fiber-tolerance checklist?
A practical fiber-tolerance checklist starts with the baseline: usual stool frequency, stool form, gas, bloating timing, water intake, and common trigger foods. Next, choose one fiber variable, such as oats at breakfast, psyllium with water, chia in yogurt, or an extra serving of kiwi. Hold the rest of the routine steady for at least several days. Record whether symptoms improve, worsen, or shift timing. If a food creates gas but improves stool form, the answer may be slower titration rather than rejection. If every high-fiber option worsens symptoms, a clinician or dietitian can help distinguish fiber intolerance from FODMAP sensitivity, constipation overflow, medication effects, or another digestive pattern. A useful log is short: food, portion, water, symptoms, stool form, and next-day comfort. The goal is pattern recognition, not perfect tracking. Three consistent observations are more useful than ten guesses.
For a detailed comparison of specific products and strains, see Bloating Every Afternoon? Compare Fiber, Probiotics, and Enzymes.
For a detailed comparison of specific products and strains, see Sunfiber for IBS-D: How PHGG Compares With Psyllium, Acacia Fiber, and Fiber Gummies.
FAQ?
Is fiber necessary for everyone?
Fiber is a normal part of a digestive-supportive diet for most people. Individual medical conditions, surgeries, bowel narrowing, or clinician-directed diets can change the right amount and type.
Why does fiber make me bloated?
Fiber can increase bloating when gut microbes ferment it quickly or when the serving size jumps too fast. Low fluid intake and constipation can also make added fiber feel heavier.
Is soluble fiber better than insoluble fiber?
Soluble fiber is often easier to titrate for sensitive digestion, especially psyllium or oat-based sources. Insoluble fiber can still support bowel movement, but coarse bran may feel rougher for some people.
Should I stop fiber if it causes gas?
Not always. First reduce the serving, change the fiber type, increase water, and slow the schedule; stop and seek medical guidance if symptoms are severe or persistent.
Are low-FODMAP diets low in fiber?
They can become low in fiber if they are poorly planned. A dietitian-guided low-FODMAP plan usually tries to preserve tolerated fiber sources while identifying specific carbohydrate triggers.
How long does fiber adaptation take?
Many people need several days to a few weeks to adapt to a higher-fiber routine. The timeline depends on baseline intake, fiber type, hydration, and gut sensitivity.
Sources: Dietary fiber in IBS review, soluble versus insoluble fiber trial, NIH fiber research summary, Monash University FODMAP resource, Johns Hopkins FODMAP overview.
Leave a Reply