A Medrol pack can coincide with gastritis-like symptoms because methylprednisolone can upset the stomach and may raise gastrointestinal bleeding risk, especially with NSAIDs, alcohol, prior ulcers, or higher-risk health history. New burning pain, nausea, black stool, vomiting blood, or worsening symptoms after steroids deserves prompt clinician review.
How did we evaluate Medrol pack induced gastritis?
We evaluated Medrol pack induced gastritis by separating documented methylprednisolone adverse effects from broader gastritis causes. We prioritized the FDA Medrol label, MedlinePlus methylprednisolone guidance, NIDDK gastritis education, and a BMJ Open systematic review over anecdotal forum reports. Human clinical evidence received more weight than single case stories because steroid timing alone cannot prove stomach-lining inflammation. This article excludes diagnosis, dosing changes, and treatment instructions because a Medrol Dosepak is a prescription taper and persistent or severe upper-abdominal symptoms need individualized medical review. The practical standard is pattern recognition: symptom onset, NSAID exposure, alcohol intake, ulcer history, and warning signs carry more value than the phrase “steroid gastritis” by itself. Evidence is strongest for gastrointestinal bleeding and perforation risk across corticosteroid trials, while evidence for short outpatient tapers causing true gastritis is more directional and context-dependent.
Can a Medrol pack cause gastritis-like symptoms?
A Medrol pack can cause gastritis-like symptoms, but it does not prove gastritis by itself. Medrol contains methylprednisolone, a corticosteroid that changes inflammation signaling throughout the body. MedlinePlus lists methylprednisolone as a medicine that can cause stomach upset and also warns against stopping it without clinician guidance. The FDA Medrol label lists gastrointestinal adverse reactions including peptic ulcer, pancreatitis, abdominal distention, ulcerative esophagitis, and stomach-related complications in susceptible patients. A short taper may feel irritating because the stomach already has reflux, NSAID exposure, alcohol exposure, Helicobacter pylori infection, or stress-related sensitivity. The timing matters: symptoms that begin soon after steroid doses and repeat after each dose make the medication a plausible contributor. Symptoms that started before the pack, continue long after it, or include alarm signs need a broader evaluation rather than a single-cause explanation.
What symptoms fit stomach irritation after methylprednisolone?
Stomach irritation after methylprednisolone usually feels like upper-abdominal burning, sour burps, nausea, early fullness, bloating, or gnawing discomfort under the breastbone. NIDDK describes gastritis and gastropathy symptoms as indigestion, pain or discomfort in the upper abdomen, nausea, vomiting, and feeling full too soon during a meal. Those symptoms overlap with reflux, dyspepsia, ulcer disease, gallbladder problems, and anxiety-related gut sensations, so symptom labels can mislead. Black, tarry stool; vomiting blood; coffee-ground vomit; faintness; severe pain; fever; chest pain; repeated vomiting; or unintended weight loss changes the situation. Those warning signs point beyond routine stomach upset and deserve urgent medical contact. Mild symptoms that track tightly with dosing still deserve a call to the prescriber, especially when the person also uses ibuprofen, naproxen, aspirin, anticoagulants, alcohol, or has a past ulcer. Age and dose history also matter.
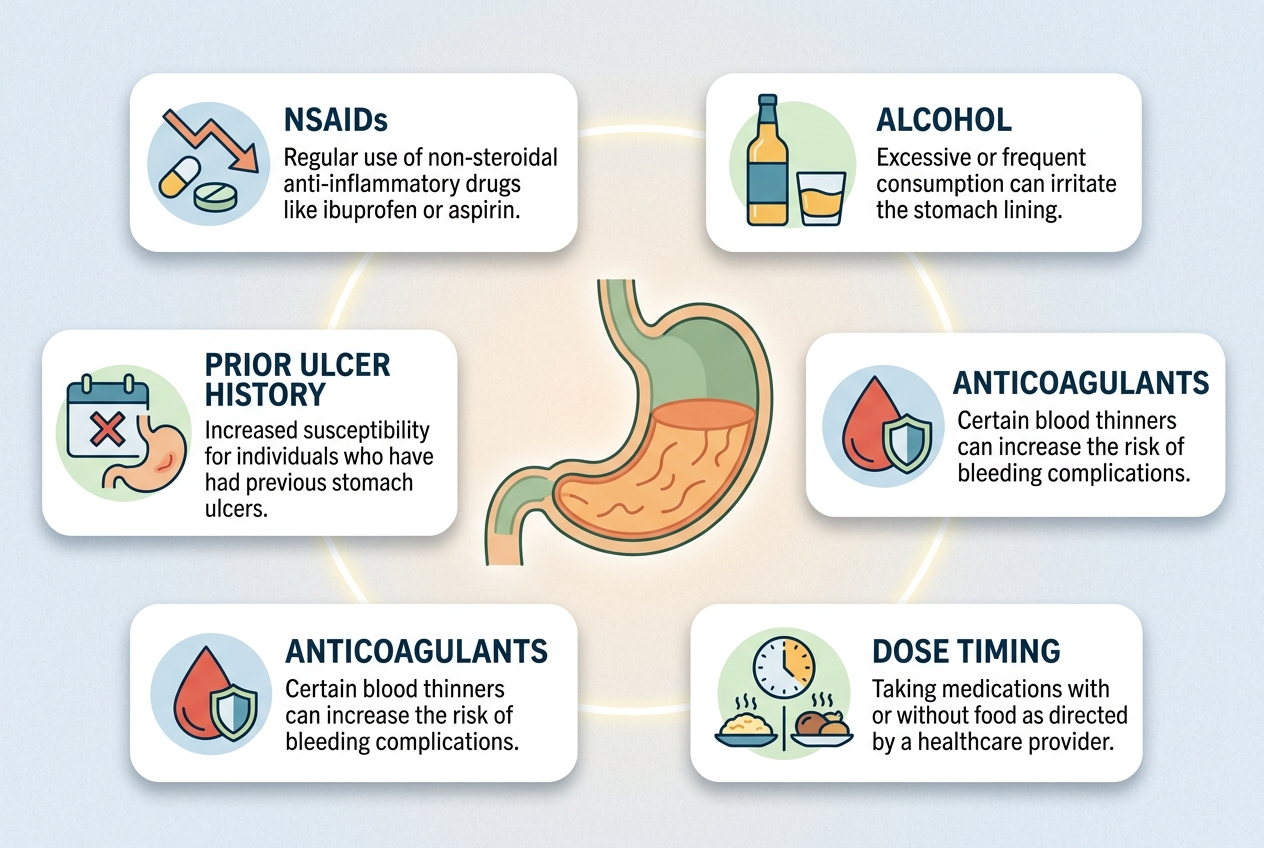
Why do NSAIDs, alcohol, and ulcer history matter so much?
NSAIDs, alcohol, and ulcer history matter because they reduce the stomach’s safety margin. The NIDDK identifies H. pylori infection and NSAID use as common causes of gastritis and gastropathy. NSAIDs such as ibuprofen, naproxen, and aspirin can weaken protective prostaglandin pathways in the gastric lining. Alcohol can irritate the lining and amplify nausea, reflux, and burning sensations. Corticosteroids add a second risk layer in some settings. A BMJ Open systematic review of randomized trials found corticosteroids increased gastrointestinal bleeding or perforation risk overall, with the clearest signal in hospitalized patients and a much lower absolute event rate in ambulatory patients. That caveat matters: a short outpatient Medrol pack is not the same exposure as high-dose inpatient steroids. Risk still rises when multiple irritants stack together. Age, anticoagulants, and ulcer history can shift that calculation.
What should you ask a clinician before changing anything?
A person with suspected Medrol-related stomach irritation should ask the prescriber what symptom pattern requires changing the plan, not guess alone. The useful details are exact dose day, timing after each tablet, pain location, nausea or reflux symptoms, NSAID use, alcohol use, ulcer history, anticoagulant use, and any black stool or vomiting. The clinician can decide whether symptoms fit expected stomach upset, reflux flare, medication interaction, ulcer concern, or a separate condition. The key safety point is the taper. MedlinePlus warns that stopping methylprednisolone abruptly can cause withdrawal-type symptoms, so schedule changes belong with the prescribing clinician. Pharmacists can also review drug interactions and stomach-irritating over-the-counter medicines. If symptoms are severe, bloody, faintness-related, or rapidly worsening, urgent care is more appropriate than waiting for a routine message. Exact wording saves time during clinical triage.
What can reduce extra stomach irritation while symptoms are being reviewed?
Extra stomach irritation often drops when avoidable triggers stop piling on top of the prescription. The safest first step is communication with the prescriber or pharmacist, because medication timing, dose schedule, and protective options depend on the reason for the steroid. While waiting for guidance, people commonly track meals, dose timing, alcohol, caffeine, spicy foods, late-night eating, and NSAID use to identify clear aggravators. Bland foods are not a treatment, but smaller low-fat meals may reduce reflux-like pressure during a sensitive week. Hydration matters because vomiting, poor appetite, and diarrhea can turn a minor stomach flare into weakness. NSAIDs deserve special caution because they are common hidden contributors to gastritis and ulcer risk. The goal is not to self-treat steroid gastritis. The goal is to lower obvious irritants and give the clinician a clean symptom timeline.
What do people get wrong about Medrol pack stomach pain?
The biggest mistake is treating “Medrol caused gastritis” as a confirmed diagnosis when it is really a timing clue. Methylprednisolone can irritate the stomach, but gastritis requires a broader context, medication reconciliation, and sometimes testing. Another mistake is adding ibuprofen or naproxen for steroid-related aches without asking a pharmacist or clinician. That combination can increase stomach risk in susceptible people. A third mistake is ignoring red-flag symptoms because the pack is short. Short courses can still reveal an existing ulcer, reflux problem, H. pylori infection, or medication interaction. A fourth mistake is stopping the taper suddenly because nausea feels scary. Prescription steroid tapers have a schedule for a reason. The better move is to document the day, dose, timing, symptoms, and other medications, then ask the prescriber what to do next. Written timelines beat anxious guessing.
For a detailed comparison of specific products and strains, see Upper Middle Stomach Pain and Bloating: Options to Compare Before Guessing.
What questions come up most often?
Is Medrol the same as methylprednisolone?
Medrol is a brand name for methylprednisolone, a corticosteroid prescription medicine. A Medrol Dosepak usually uses a short tapering schedule, so dose timing and stopping decisions should follow the prescriber’s instructions.
Can a short steroid pack cause real gastritis?
A short steroid pack can contribute to stomach irritation, but true gastritis is not automatic. NSAID use, alcohol, H. pylori infection, prior ulcers, and baseline reflux can make the same steroid week feel much worse.
Is burning pain after each dose a useful clue?
Yes. Burning that starts after each dose and improves between doses makes medication irritation plausible. It still does not rule out reflux, ulcer disease, gallbladder problems, or another cause.
Should NSAIDs be avoided during a Medrol pack?
NSAIDs deserve a clinician or pharmacist check during steroid use, especially when stomach symptoms appear. Ibuprofen, naproxen, and aspirin can irritate the stomach lining and may compound risk in people with ulcer history.
When is this urgent?
Black stool, vomiting blood, coffee-ground vomit, faintness, severe abdominal pain, chest pain, repeated vomiting, or rapidly worsening symptoms deserves urgent medical help. Those signs are not routine “stomach upset.”
Can antacids or acid reducers be used with methylprednisolone?
Only a clinician or pharmacist should confirm what fits your medication list and steroid schedule. Antacids, H2 blockers, and proton pump inhibitors have different timing rules, interaction concerns, and reasons for use.
What information should be included in a message to the prescriber?
Include the Medrol day and dose, symptom start time, pain location, nausea or reflux symptoms, NSAID or aspirin use, alcohol use, ulcer history, and any black stool or vomiting. That timeline lets the clinician sort irritation from warning signs faster.
Leave a Reply