H. pylori ulcers, non-H. pylori ulcers, and GERD can overlap, but they do not follow the same pattern. Without endoscopy, symptom timing, alarm signs, medication response, and noninvasive H. pylori testing can guide the next step. Persistent pain, bleeding signs, weight loss, vomiting, or anemia need medical evaluation.
How did we evaluate H. pylori, ulcer, and GERD clues?
We evaluated this question by prioritizing clinical pattern recognition, noninvasive testing, and safety flags rather than home diagnosis. American College of Gastroenterology guidance, Mayo Clinic symptom summaries, and peer-reviewed reviews received more weight than forum anecdotes. Endoscopy remains the definitive tool for many ulcer and reflux complications, so this article focuses on what can be reasonably sorted before that point. The goal is triage clarity, not self-treatment or a replacement for a clinician.
Can symptoms alone separate H. pylori, an ulcer, and GERD?
Symptoms alone cannot reliably separate H. pylori infection, a peptic ulcer, and GERD because upper-abdominal burning, nausea, burping, early fullness, and chest discomfort can overlap. GERD usually centers on acid reflux into the esophagus, so heartburn, sour regurgitation, throat irritation, and worse symptoms after lying down point toward reflux physiology. Peptic-ulcer pain more often sits in the upper abdomen and may relate to meals, NSAID use, or night discomfort. H. pylori is a bacterium associated with some ulcers, but many infected people have no symptoms. Mayo Clinic describes peptic-ulcer symptoms as burning stomach pain, bloating, belching, and intolerance to fatty foods, while GERD symptoms often include heartburn and regurgitation. The safe answer is pattern-based: symptoms can suggest a direction, but testing decides more than sensation does.
What noninvasive tests help before endoscopy?
Noninvasive H. pylori testing can clarify one major branch before endoscopy. The American College of Gastroenterology describes urea breath testing, stool antigen testing, and certain laboratory-based tests as useful options for detecting active H. pylori infection (ACG guideline). Test accuracy depends on preparation because proton pump inhibitors, bismuth, and antibiotics can cause false negatives if used too close to testing. A clinician usually gives a washout window before a breath or stool test. Blood antibody tests are less useful for active infection because antibodies can remain after past exposure. GERD does not have one simple home-equivalent test; response to lifestyle changes or acid-suppressing medication can provide clues, but response does not prove the diagnosis. If symptoms persist, recur, or include alarm signs, endoscopy or additional evaluation may be appropriate.
Which pattern points more toward reflux?
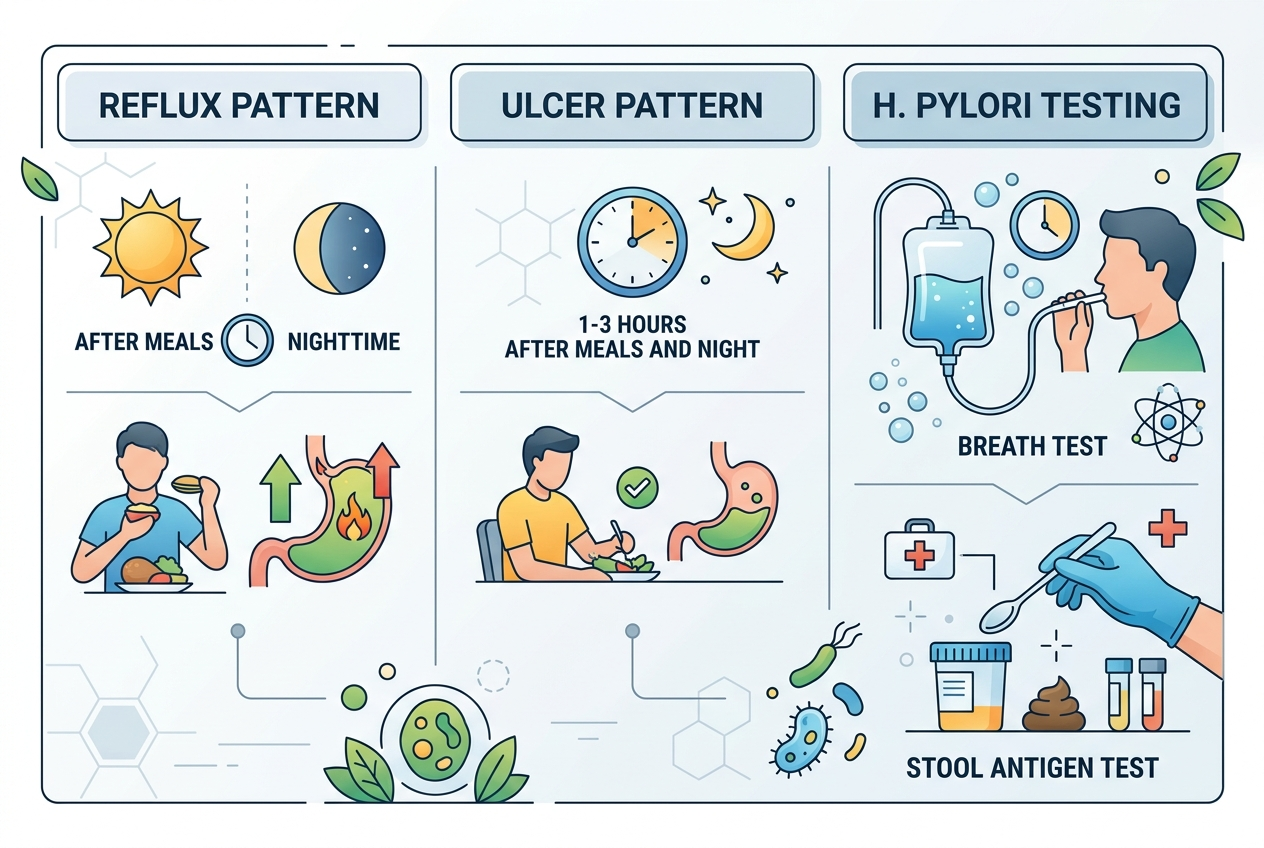
A reflux pattern usually involves burning behind the breastbone, sour or bitter regurgitation, symptoms after large or late meals, and worsening when lying down or bending. GERD reflects stomach contents moving into the esophagus, not an ulcer sitting in the stomach lining. Johns Hopkins Medicine notes that GERD can cause heartburn, regurgitation, chest discomfort, throat symptoms, and swallowing issues in some people (Johns Hopkins). A reflux diary should track meal timing, caffeine, alcohol, chocolate, mint, high-fat meals, late-night snacks, sleep position, and symptom timing. Improvement with earlier dinners, head-of-bed elevation, smaller meals, or clinician-guided acid suppression supports reflux as a working pattern. It does not rule out ulcer disease, gallbladder issues, cardiac causes, or H. pylori. Chest pain, trouble swallowing, vomiting blood, black stool, or unexplained weight loss needs prompt care.
Which pattern points more toward an ulcer or H. pylori?
An ulcer pattern usually involves gnawing or burning upper-abdominal pain, nighttime pain, nausea, early fullness, or discomfort that changes with food. H. pylori and NSAID medications are two major peptic-ulcer drivers. The National Institute of Diabetes and Digestive and Kidney Diseases states that H. pylori infection and long-term NSAID use are common causes of peptic ulcers (NIDDK). A person should note ibuprofen, naproxen, aspirin, corticosteroids, anticoagulants, alcohol intake, and prior ulcer history before assuming reflux. Black tarry stool, vomiting blood, faintness, severe persistent pain, or anemia symptoms can signal bleeding and require urgent evaluation. H. pylori is treatable when confirmed, but treatment requires an appropriate antibiotic regimen and confirmation of eradication. Guessing with supplements or antacids can delay the test that matters.
What should you track before a clinician visit?
A useful pre-visit log captures timing, location, triggers, medication use, and red flags. Track whether discomfort sits behind the breastbone, under the ribs, or in the upper abdomen. Record whether symptoms occur before meals, after meals, overnight, during exercise, or when lying down. List NSAIDs, aspirin, steroids, iron, potassium, antibiotics, antacids, H2 blockers, proton pump inhibitors, alcohol, nicotine, and caffeine. Note stool color, vomiting, fever, weight change, swallowing trouble, shortness of breath, and chest pressure. Bring prior test results, H. pylori history, endoscopy history, and family history of ulcer disease or gastrointestinal cancer. This structured log helps a clinician choose between H. pylori testing, medication adjustment, reflux evaluation, lab work, imaging, or endoscopy.
For a detailed comparison of specific products and strains, see What to Do if You Have Chronic Acid Reflux: Which Support Options Actually Make Sense?.
What questions do people ask about H. pylori, ulcers, and GERD?
Can H. pylori feel exactly like GERD?
Yes. H. pylori-associated gastritis or ulcers can create burning, nausea, burping, and upper-abdominal discomfort that feels similar to reflux. Testing is more reliable than symptom guessing.
Can GERD happen without heartburn?
Yes. Some reflux patterns cause throat clearing, sour taste, cough, hoarseness, nausea, or chest discomfort without classic heartburn. Persistent or unusual symptoms still need evaluation.
Does a PPI response prove GERD?
No. PPI response can support an acid-related pattern, but it does not prove GERD or exclude ulcer disease. PPIs can also interfere with H. pylori testing if used too close to the test.
When is endoscopy more important?
Endoscopy becomes more important with bleeding signs, anemia, trouble swallowing, persistent vomiting, unintentional weight loss, severe pain, or symptoms that do not respond as expected. Age and risk factors also influence the threshold.
Can stress alone cause an ulcer?
Ordinary daily stress is not the classic cause of peptic ulcers. H. pylori and NSAID use are better-supported causes, although stress can worsen symptom perception and reflux behaviors.
What is the safest next step if I cannot tell?
The safest next step is to document the pattern and ask about H. pylori breath or stool testing, medication review, and alarm signs. If symptoms are severe or include bleeding signs, urgent care is safer than waiting.
Leave a Reply