A 2026 pilot trial suggests probiotics may improve semen concentration, motility, and morphology more than antioxidants or placebo in men with unexplained abnormal semen parameters. The finding is promising but not settled. Probiotics should be viewed as an investigational fertility-support strategy that needs larger trials, clinician oversight, and standard semen analysis follow-up.
How we evaluated probiotics and sperm quality?
We evaluated this topic by prioritizing human randomized trials, systematic reviews, clinical-trial records, and fertility-organization context over supplement marketing claims. Semen concentration, motility, morphology, DNA fragmentation, and pregnancy outcomes were treated as separate endpoints because an improvement in one laboratory marker does not prove improved live-birth probability. We excluded animal-only mechanisms from the core answer unless they explained a hypothesis already tested in humans. The main limitation is that probiotic fertility research remains small, heterogeneous, and early compared with established fertility evaluation pathways. We also treated semen analysis as a clinical test, not a consumer wellness score, because laboratory interpretation depends on collection timing, abstinence interval, repeat samples, and medical history.
What did the 2026 probiotic sperm-quality study find?
The 2026 randomized pilot trial published in PubMed Central reported that probiotic supplementation improved sperm concentration, motility, and morphology compared with baseline, placebo, and antioxidant supplementation in men with idiopathic oligoasthenoteratozoospermia. The study’s conclusion says both probiotics and antioxidants improved semen parameters, but probiotics showed stronger gains across the measured semen-quality markers. That result supports a hypothesis, not a final treatment rule. Pilot trials can overestimate effect size because sample sizes are small, participant selection is narrow, and follow-up windows are limited. The most useful takeaway is specific: probiotic exposure may influence measurable semen parameters in some men with unexplained low count, weak motility, or abnormal morphology. The least useful takeaway is broad: “probiotics fix sperm quality.” The evidence does not support that stronger claim, especially without pregnancy-outcome data.
Why might gut bacteria affect sperm quality?
Researchers propose several gut-reproductive links, but none should be treated as proven for every person. The gut microbiome can influence systemic inflammation, oxidative stress signaling, nutrient metabolism, and immune activity. Those pathways can theoretically affect testicular function and semen quality because sperm development is sensitive to oxidative stress and inflammatory burden. A 2026 systematic review in Urologia Colombiana found promising probiotic effects on semen concentration, volume, and motility, but the review included only four studies and reported high heterogeneity. That means the pooled result is directionally interesting, not definitive. The strongest current explanation is modest: probiotic strains may support a healthier inflammatory and oxidative environment in some men. The weaker explanation is causal certainty, because strain choice, diet, antibiotics, sleep, smoking, varicocele status, and baseline microbiome differences can all change outcomes.
How do probiotics compare with antioxidants for semen parameters?
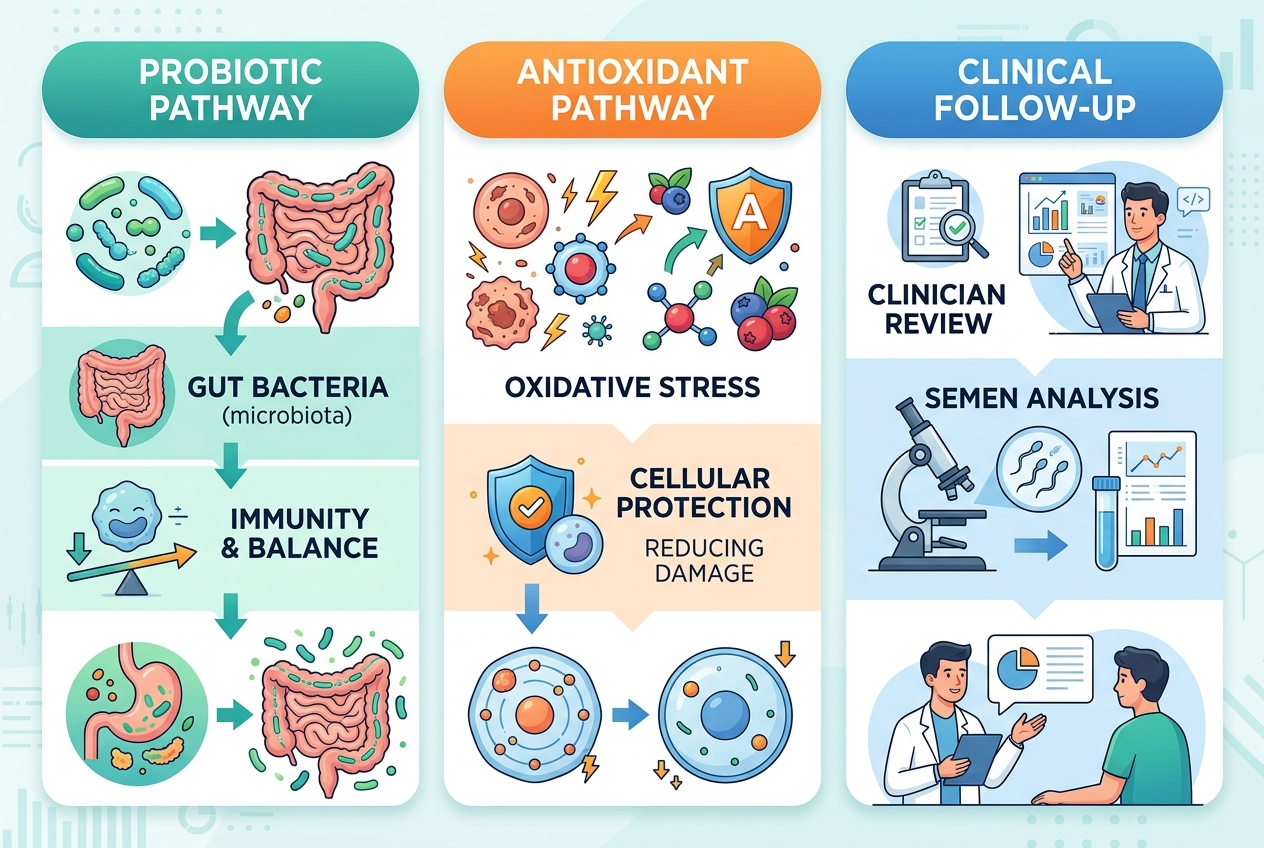
Antioxidants and probiotics target overlapping but different hypotheses. Antioxidants target oxidative stress directly by supplying compounds such as vitamin C, vitamin E, zinc, selenium, coenzyme Q10, or alpha-lipoic acid. Probiotics target microbial ecology and downstream immune or metabolic signaling, which may indirectly influence oxidative stress. A Cochrane review on antioxidants for male subfertility found possible improvements in live birth and clinical pregnancy, but the evidence quality was low or very low for many outcomes. The 2026 probiotic pilot trial is notable because it compared probiotics with antioxidants and placebo in the same study design. That comparison makes probiotics worth studying, but it does not make antioxidants obsolete. Fertility clinicians still need context such as semen analysis repeatability, hormonal testing, varicocele evaluation, medication review, and reproductive-timeline goals before recommending any supplement plan.
What should someone do with this information?
Someone reading the probiotic study should use it as a conversation starter, not a self-treatment protocol. A semen analysis can vary from sample to sample, so clinicians usually interpret sperm concentration, motility, and morphology alongside repeat testing and medical history. The World Health Organization semen-analysis manual standardizes laboratory assessment, but a lab result still needs clinical context. Men with abnormal semen parameters should ask a reproductive urologist or fertility clinician whether probiotics, antioxidants, diet changes, smoking cessation, heat avoidance, medication review, or varicocele evaluation fits their case. Probiotics are generally marketed as supplements, but supplement quality, strain identity, CFU viability, and storage conditions differ widely. The safest interpretation is that probiotics may be a reasonable research-backed topic to discuss after abnormal semen analysis, especially when the abnormality is unexplained.
What do people get wrong about probiotic fertility claims?
The first mistake is turning “improved semen parameters” into “improved fertility.” Semen concentration, motility, and morphology are important laboratory markers, but pregnancy and live birth depend on both partners, timing, ovulation, tubal factors, age, genetics, and clinical treatment choices. The second mistake is assuming every probiotic product matches the strains, dose, or duration used in a study. Probiotic effects are strain-specific, and broad genus names such as Lactobacillus or Bifidobacterium do not identify a finished product. The third mistake is treating antioxidants and probiotics as an either-or decision. Some men may benefit from lifestyle changes, targeted supplementation, medical treatment, or no supplement at all. The fourth mistake is ignoring repeat semen analysis, because one abnormal sample can mislead decision-making. The evidence supports measured curiosity, not a shortcut around fertility evaluation.
For a detailed comparison of specific products and strains, see Best Probiotics for Men’s Gut Health in 2026: What to Compare.
What should readers ask before trying probiotics for sperm quality?
Does the 2026 study prove probiotics improve male fertility?
No. The 2026 study reported improvements in semen parameters, not proof of higher pregnancy or live-birth rates. The result is clinically interesting because semen concentration, motility, and morphology are relevant fertility markers, but the endpoint is still indirect.
Are probiotics better than antioxidants for sperm quality?
One 2026 pilot trial found stronger semen-parameter improvements with probiotics than antioxidants, but one pilot trial cannot settle the comparison. Antioxidant evidence also remains mixed, and Cochrane reviewers have rated much of the pregnancy-outcome evidence as low quality. Clinician guidance matters.
Which probiotic strain is best for sperm quality?
The evidence does not yet support one universal “best” strain. Trials use different formulas, doses, durations, and populations. A responsible review should match claims to the exact studied strain or finished formula when that information is available.
How long would probiotics take to affect semen analysis?
Human sperm development takes roughly several months, so fertility studies often use multi-week or multi-month interventions. A single week of probiotic use is unlikely to provide a meaningful semen-analysis conclusion. Repeat testing should follow a clinician’s timing.
Can diet do the same thing as probiotics?
Diet and fiber intake can influence the gut microbiome, but diet is not identical to a probiotic supplement. Whole-food patterns may support metabolic and inflammatory health, while probiotic capsules or fermented foods deliver specific live organisms. The two strategies can overlap.
Should someone stop prescribed fertility treatment and take probiotics instead?
No. Probiotics should not replace reproductive-urology evaluation, hormonal assessment, varicocele workup, medication review, or assisted-reproduction planning. Supplements can also interact with medical priorities, so abnormal semen parameters deserve professional follow-up.
Are probiotics safe for everyone?
Most healthy adults tolerate common probiotics, but risk is higher for people who are severely immunocompromised, have central venous catheters, or have complex medical conditions. Anyone in a fertility workup should disclose supplements to the clinician reading the semen-analysis results.