
GERD is more likely when reflux symptoms happen repeatedly, appear at night, wake you from sleep, cause sour regurgitation, or continue despite changing meals. A bad diet is more likely when burning follows specific triggers such as large portions, alcohol, coffee, high-fat foods, late eating, or lying down soon after dinner.
How did we evaluate whether symptoms point to GERD or diet?
This article evaluated reflux patterns using gastroenterology guidelines, government digestive-health references, and symptom-timing logic rather than single-food blame. Human clinical guidance from the American College of Gastroenterology and the National Institute of Diabetes and Digestive and Kidney Diseases received more weight than anecdotes from forums or wellness blogs. Diet claims were included only when they matched recurring mechanisms: stomach distension after large meals, lower esophageal sphincter relaxation after alcohol or high-fat meals, delayed gastric emptying, or reflux after lying flat. Food-list claims were treated as individual trigger hypotheses, not universal rules, because reflux patterns vary across bodies and contexts. The main limitation is that symptom patterns cannot confirm GERD, esophagitis, eosinophilic esophagitis, ulcer disease, gallbladder disease, or cardiac causes; a clinician uses history, response patterns, medication review, and sometimes endoscopy or pH monitoring to separate those possibilities.
What patterns make GERD more likely than ordinary food-related reflux?
GERD becomes more likely when acid reflux symptoms form a repeated pattern rather than a one-off reaction to a heavy meal. The National Institute of Diabetes and Digestive and Kidney Diseases defines GERD as a chronic condition in which stomach contents repeatedly flow back into the esophagus and cause symptoms or complications. Heartburn more than occasional, sour regurgitation, chest burning after lying down, hoarseness, chronic cough, throat clearing, and sleep disruption all point toward reflux that is not purely about one poor food choice. The American College of Gastroenterology guideline notes that typical heartburn and regurgitation often guide initial clinical evaluation, while alarm symptoms change the workup. Diet can still aggravate GERD, but a persistent baseline pattern suggests an underlying reflux tendency. A food-trigger pattern explains episodes; a recurring night, regurgitation, or sleep pattern raises the GERD suspicion.
What patterns make diet or eating habits the more likely driver?
Diet becomes the more likely driver when symptoms track closely with timing, portions, and specific triggers. Large meals increase stomach pressure, late meals place a full stomach near bedtime, and lying flat removes gravity from the reflux equation. Alcohol, peppermint, coffee, chocolate, high-fat meals, spicy foods, tomato-based foods, and citrus can bother some people, but the National Institute of Diabetes and Digestive and Kidney Diseases emphasizes that triggers vary by person rather than following one universal list. A bad-week pattern also matters: travel meals, fast food, lower fiber intake, carbonated drinks, stress eating, and rushed dinners can cluster into several reflux episodes without proving chronic GERD. If symptoms disappear after two weeks of smaller dinners, earlier eating, lower alcohol intake, and fewer high-fat meals, eating habits become the stronger explanation. If symptoms continue, diet may be an aggravator rather than the root pattern.
When should symptoms be checked by a clinician?
Symptoms should be checked promptly when reflux overlaps with trouble swallowing, painful swallowing, vomiting blood, black stools, unexplained weight loss, anemia, persistent vomiting, or chest pain. The American College of Gastroenterology guideline handles these alarm features differently from uncomplicated heartburn because they can signal esophageal injury or non-reflux conditions. Chest pressure, shortness of breath, sweating, jaw pain, or arm pain needs urgent medical evaluation because heart-related pain can mimic indigestion. A clinician should also review symptoms that occur several times per week, wake you regularly, return after over-the-counter acid reducers, or require frequent medication. GERD is common, but common does not mean self-labeled. A careful medical history separates reflux from medication side effects, pregnancy-related reflux, functional dyspepsia, peptic ulcer disease, gallbladder disease, eosinophilic esophagitis, and cardiac conditions. Pattern tracking helps the appointment; it does not replace evaluation when warning signs appear.
What can you track for two weeks before assuming one cause?
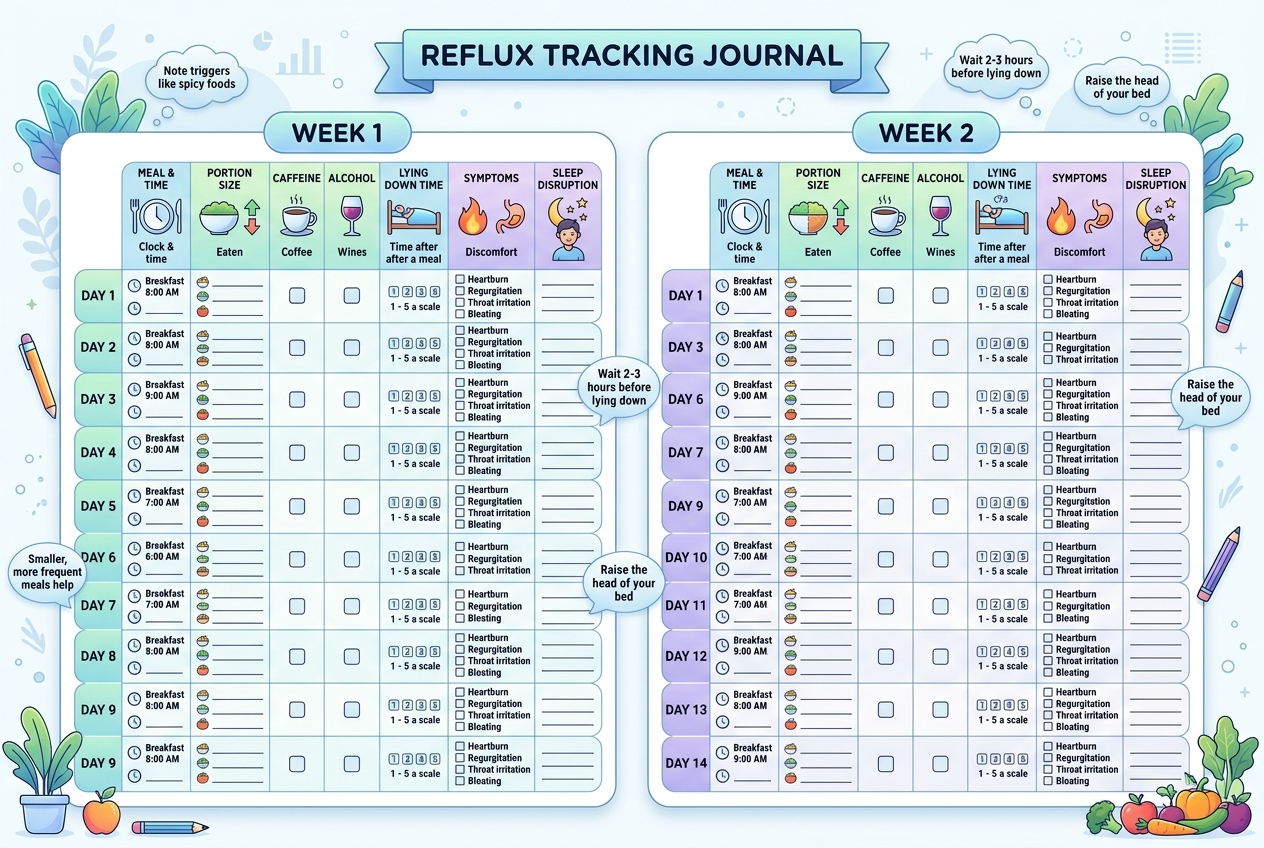
A two-week reflux log should track symptom time, last meal time, portion size, alcohol, caffeine, carbonation, high-fat foods, spicy foods, tomato or citrus foods, lying-down time, exercise, stress, sleep position, and medication use. The goal is pattern detection, not perfection. A 0-to-10 score for each symptom makes the data easier to compare. Strong clues include symptoms within two hours of dinner, symptoms after meals larger than usual, symptoms after alcohol plus late eating, and symptoms that improve when dinner moves three or more hours before bed. The ACG guideline gives stronger support to weight management and avoiding meals close to bedtime than to eliminating every possible trigger, while a 2021 JAMA Internal Medicine cohort analysis reported lifestyle associations rather than proof that one food causes reflux in every person. A useful log therefore tests the highest-probability behaviors first. If symptoms stay frequent despite a cleaner pattern, GERD or another medical cause deserves a closer look.
For a detailed comparison of specific products and strains, see Gallbladder or GERD? How to Tell the Difference and What to Do About It.
What questions do people ask about GERD versus diet?
Can a bad diet cause GERD?
A bad diet can aggravate reflux symptoms, but it does not prove GERD by itself. GERD usually means a repeated reflux pattern that persists beyond occasional trigger meals.
Can GERD happen even if I eat healthy food?
GERD can happen with a careful diet because reflux involves anatomy, pressure, stomach emptying, sleep position, medications, pregnancy, weight changes, and lower esophageal sphincter function. Healthy meals can still trigger symptoms if portions are large or bedtime follows too soon.
How many reflux episodes are normal?
Occasional heartburn after a large or late meal is common. Reflux that appears several times per week, disrupts sleep, or includes regurgitation deserves more attention.
Is coffee always bad for reflux?
Coffee is not a universal reflux trigger. A two-week log can show whether coffee alone matters, or whether symptoms depend on coffee plus an empty stomach, stress, alcohol, or late meals.
Does spicy food mean I have GERD?
Spicy food can irritate symptoms in some people, but spicy food does not confirm GERD. A repeated pattern across non-spicy meals is more suspicious than one reaction after a hot meal.
Should I cut out every acidic food?
Cutting out every acidic food is usually less useful than testing likely triggers one at a time. Smaller dinners, earlier eating, lower alcohol intake, and fewer high-fat meals often provide clearer evidence.
What is the clearest sign that it is not just diet?
The clearest sign is persistence despite consistent meal changes. Night symptoms, sour regurgitation, swallowing problems, or frequent symptoms despite smaller earlier meals point beyond ordinary dietary irritation.
Leave a Reply