Antidepressants are sometimes prescribed for GERD-like symptoms because low-dose neuromodulators can reduce esophageal pain sensitivity, reflux hypersensitivity, functional heartburn, or gut-brain signaling when acid suppression alone does not explain symptoms. The prescription does not necessarily mean the clinician thinks the reflux is “all in your head.”
How did we evaluate antidepressants for GERD-like symptoms?
We evaluated this topic through gastroenterology guidelines, esophageal testing references, and clinical trials on functional heartburn and reflux hypersensitivity. We prioritized American College of Gastroenterology guidance, PubMed-indexed trials, and physiology-based explanations over forum anecdotes or medication marketing. We excluded personal dosing advice because antidepressants, proton pump inhibitors, H2 blockers, and anxiety medications require individualized prescribing. The key distinction is clinical: classic GERD involves abnormal reflux burden, while reflux hypersensitivity and functional heartburn involve symptom perception, nerve signaling, or symptom association with normal acid exposure.
Why would a GERD clinician prescribe an antidepressant?
A clinician may prescribe a low-dose antidepressant for GERD-like symptoms when reflux testing, endoscopy, PPI response, and symptom pattern suggest esophageal hypersensitivity or functional heartburn. The 2022 American College of Gastroenterology GERD guideline says ambulatory reflux monitoring can help establish or refute GERD and correlate symptoms with reflux episodes (ACG GERD guideline). When acid exposure is normal but symptoms remain intense, the treatment target may shift from acid quantity to nerve sensitivity. Tricyclic antidepressants, selective serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors, or related neuromodulators can be used at doses different from depression treatment. The goal is symptom modulation, not personality change. That is why a prescription can appear surprising: the drug class name describes one use, while the digestive use targets visceral pain pathways and brain-gut signaling.
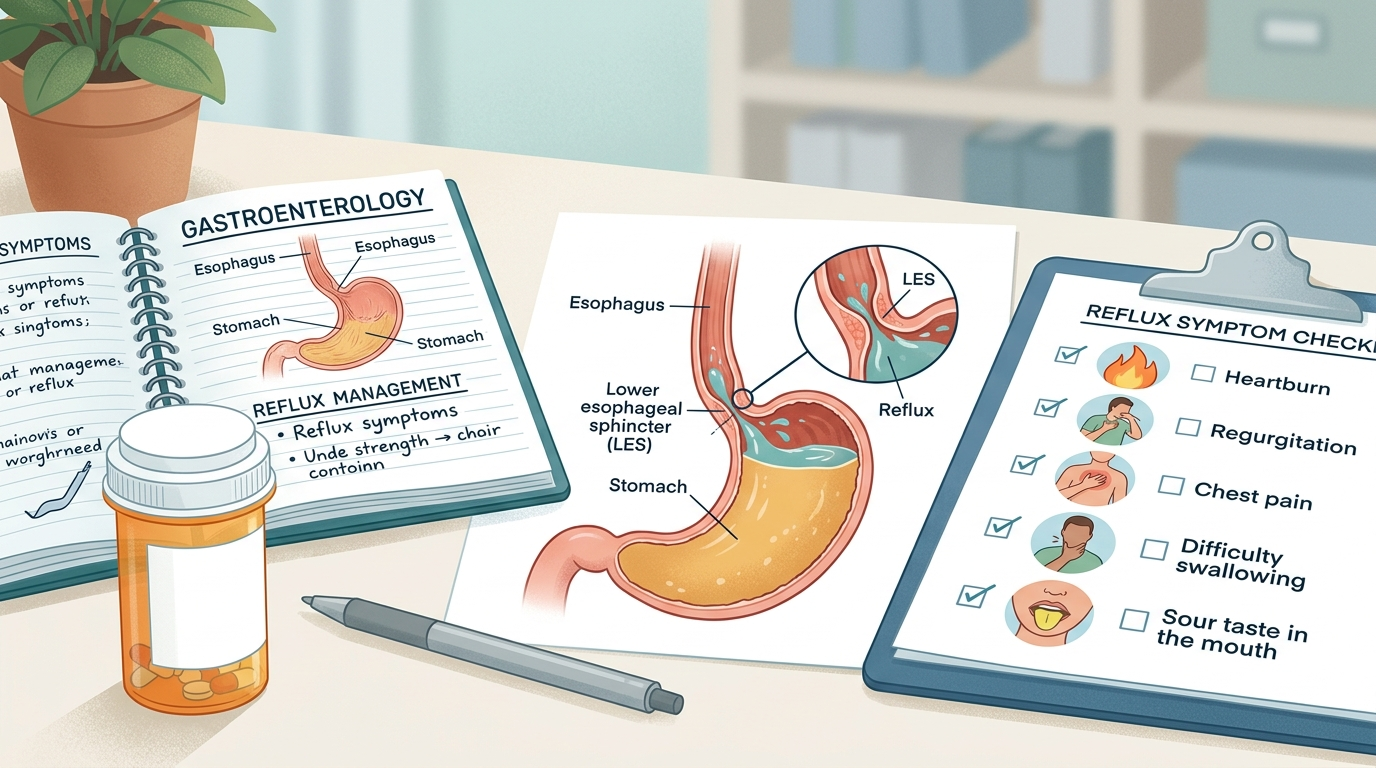
What is reflux hypersensitivity?
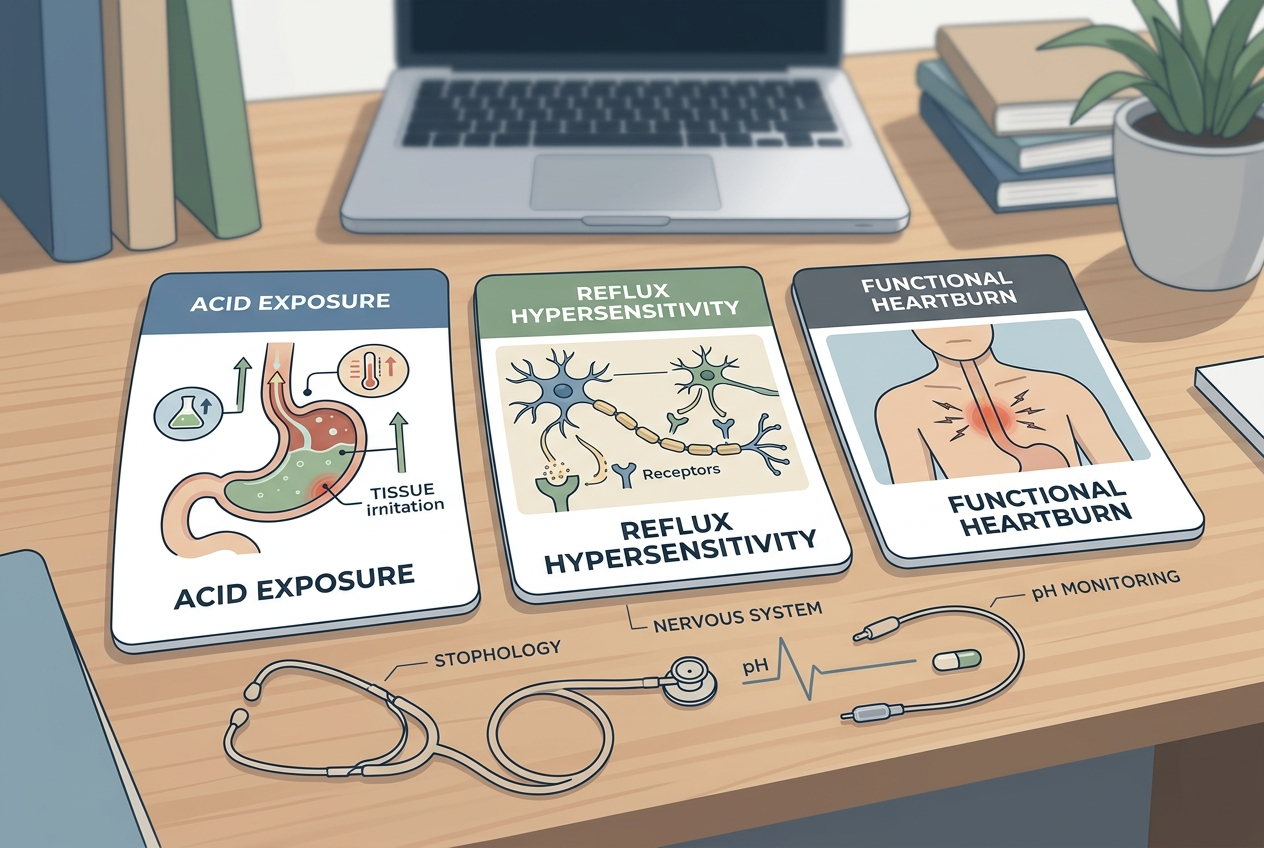
Reflux hypersensitivity means normal or near-normal reflux events create symptoms because the esophagus reacts strongly to stimuli that would not bother another person. ACG physiologic testing guidance says endoscopy, reflux monitoring, and manometry can help separate GERD, structural disorders, motor disorders, behavioral syndromes, and functional esophageal disorders (ACG esophageal testing guideline). Reflux hypersensitivity is not imaginary. The esophagus contains sensory nerves, smooth muscle, immune cells, and epithelial barriers that can change symptom perception. A person can feel burning, chest discomfort, throat sensation, or regurgitation-like distress even when acid exposure does not meet classic GERD thresholds. The practical difference matters because more acid suppression may not solve a sensitivity-driven pattern. A clinician may choose a neuromodulator when the symptom generator looks more like sensory amplification than ongoing corrosive acid exposure.
How is functional heartburn different from GERD?
Functional heartburn describes heartburn symptoms without abnormal acid exposure, without clear symptom-reflux association, and without visible esophageal injury on standard evaluation. Classic GERD usually shows erosive esophagitis, abnormal acid exposure, or symptom improvement that tracks acid suppression. Functional heartburn belongs to disorders of gut-brain interaction, where pain processing, hypervigilance, stress physiology, and esophageal sensitivity can maintain symptoms. A randomized placebo-controlled trial of imipramine in esophageal hypersensitivity and functional heartburn tested whether a tricyclic antidepressant could reduce symptoms through pain modulation rather than acid reduction (Limsrivilai et al., American Journal of Gastroenterology). The evidence is mixed and not a universal answer. The important point is classification. If symptoms persist despite appropriate GERD therapy, a clinician may investigate whether acid, motility, anatomy, or nerve sensitivity is driving the pattern.
What should you ask before taking it?
Ask the prescriber what diagnosis the medication is targeting, what test results support that diagnosis, what dose is being used, and what outcome should change first. Ask whether the goal is reflux hypersensitivity, functional heartburn, functional dyspepsia, anxiety-associated symptom amplification, sleep support, or another reason. Ask how long the trial should last, how side effects will be handled, and whether the medication interacts with PPIs, H2 blockers, antacids, SSRIs, sleep aids, alcohol, or other prescriptions. Ask what symptoms require urgent care, such as trouble swallowing, vomiting blood, black stool, severe chest pain, unexplained weight loss, anemia, or persistent vomiting. These questions do not challenge the clinician; they clarify the treatment target. A good explanation should connect the prescription to a specific symptom mechanism, not leave the patient guessing.
What are the common options doctors compare?
Doctors may compare acid suppression, lifestyle measures, reflux testing, motility evaluation, behavioral therapy, and neuromodulators depending on the pattern. Proton pump inhibitors reduce stomach acid and fit confirmed acid-mediated GERD. H2 blockers reduce acid through a different mechanism and may fit milder or nighttime patterns. Neuromodulators target pain signaling and fit selected cases of reflux hypersensitivity, functional heartburn, or overlapping gut-brain disorders. Behavioral approaches can reduce rumination, supragastric belching, hypervigilance, and stress-linked symptom loops when those mechanisms are present. Procedures are usually reserved for carefully documented reflux or anatomy problems because sensitivity-driven symptoms may not improve after anti-reflux surgery. The ACG GERD guideline emphasizes objective evaluation before invasive therapy in unclear cases (ACG full guideline). The best option depends on evidence, not symptom intensity alone.
What questions do people ask about antidepressants for GERD?
Does this mean my GERD is caused by anxiety?
No. A neuromodulator prescription can mean the clinician suspects nerve sensitivity, reflux hypersensitivity, or functional heartburn. Anxiety may amplify symptoms in some people, but it is not the only reason these medicines are used.
Are low-dose antidepressants the same as depression treatment?
Not always. Gastroenterologists often use lower doses for pain modulation than psychiatrists use for major depression. The prescriber should explain the dose, expected timeline, and side effect plan.
Should I stop my PPI if I start a neuromodulator?
Do not stop prescribed medicine without the clinician’s plan. Some people use acid suppression and neuromodulation together while diagnostic clarity improves.
What tests clarify the diagnosis?
Endoscopy, ambulatory pH monitoring, impedance-pH monitoring, and esophageal manometry can clarify acid exposure, symptom association, motility, and functional patterns. The exact test depends on symptoms and prior results.
When should symptoms be urgent?
Chest pain, trouble swallowing, vomiting blood, black stool, fainting, severe abdominal pain, anemia, or unintended weight loss deserves prompt medical attention. Those signs should not be managed as routine reflux.
Can supplements replace this treatment?
No supplement should replace a prescribed neuromodulator, PPI, or diagnostic plan. Supplements may support general routines, but they do not diagnose reflux hypersensitivity or functional heartburn.
What is the practical next step?
The practical next step is to ask for the working diagnosis in plain language: GERD, reflux hypersensitivity, functional heartburn, functional dyspepsia, anxiety-linked symptom amplification, or another condition. Then ask what evidence supports that label and what improvement should appear during the medication trial. A prescription makes more sense when the mechanism is named.
Leave a Reply