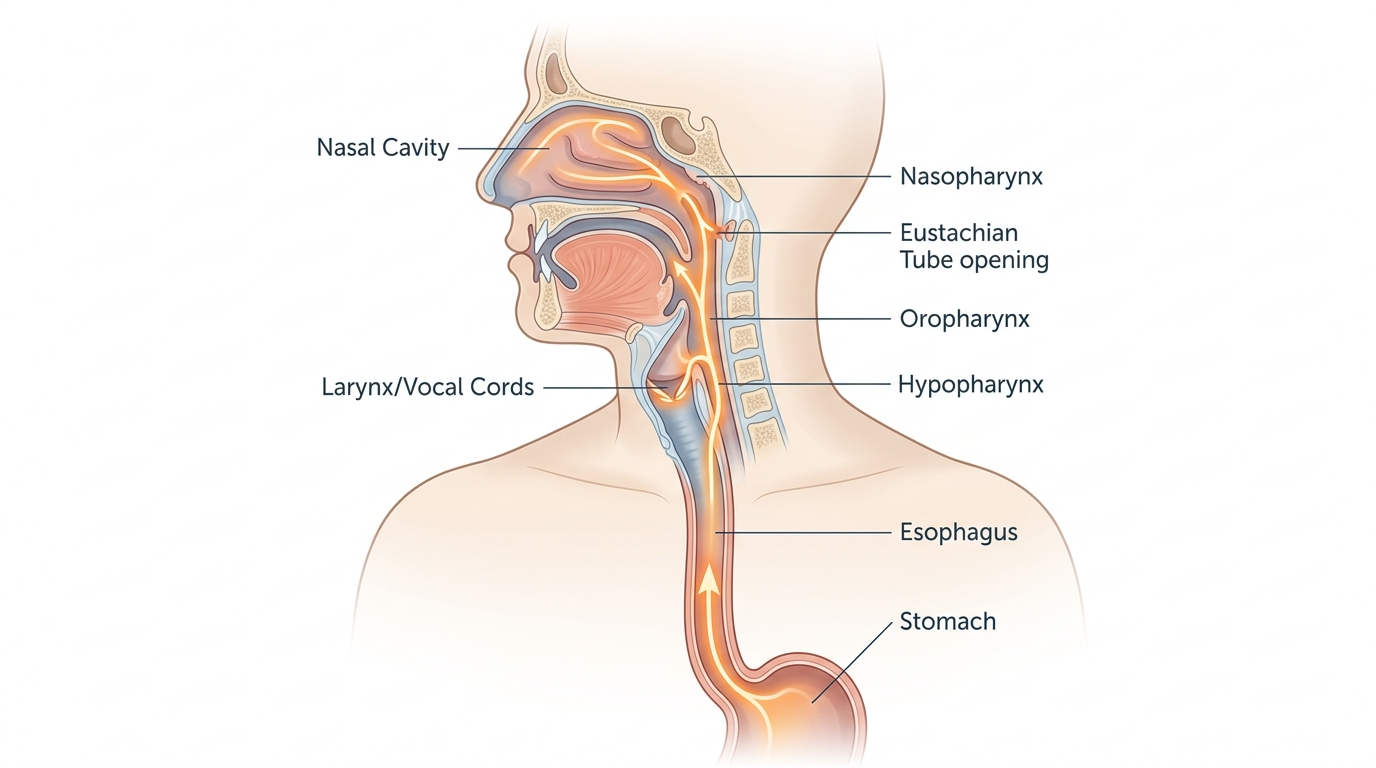
Acid reaching the ears, nose, and throat signals laryngopharyngeal reflux (LPR), a condition where stomach acid and digestive enzymes travel past both the lower and upper esophageal sphincters into the pharynx and nasal cavity. To reduce it: elevate the head of your bed 6–8 inches, avoid eating 2–3 hours before lying down, and limit acidic, fatty, and caffeinated foods.
How we evaluated this topic
This article draws on clinical guidelines from the American Academy of Otolaryngology–Head and Neck Surgery, peer-reviewed research published in Laryngoscope, Otolaryngology–Head and Neck Surgery, and data from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Priority was given to prospective human trials and systematic reviews over case reports. Industry-funded studies without independent replication were excluded. This article is educational and does not replace clinical evaluation; LPR diagnosis requires assessment by a physician or ENT specialist.
What is laryngopharyngeal reflux and how does acid reach the throat, nose, and ears?
Laryngopharyngeal reflux (LPR) occurs when gastric acid and the enzyme pepsin travel beyond the lower esophageal sphincter (LES) and upper esophageal sphincter (UES) into the pharynx, larynx, nasal passages, and Eustachian tubes connecting to the middle ear. Unlike gastroesophageal reflux disease (GERD), LPR often presents without heartburn—clinicians call this “silent reflux.” Pepsin retains enzymatic activity at pH levels as low as 4.0, meaning it continues irritating mucosal tissue in the throat and nasal passages long after acid exposure. When refluxate reaches the Eustachian tube, it can cause ear fullness, muffled hearing, or popping. The American Academy of Otolaryngology–Head and Neck Surgery estimates LPR affects approximately 10% of adults referred to ENT specialists.
- LPR mechanism: acid and pepsin bypass both esophageal sphincters
- Pepsin: active at pH 4.0, damaging to throat and nasal mucosa
- Eustachian tube involvement: explains ear symptoms in LPR patients
How does LPR differ from typical acid reflux (GERD)?
GERD and LPR share a common cause—compromised sphincter function—but they produce different symptom profiles. GERD primarily causes heartburn, regurgitation, and chest discomfort because acid pools in the esophagus. LPR symptoms concentrate in the upper aerodigestive tract: chronic throat clearing, hoarseness, postnasal drip, a sensation of a lump in the throat (globus pharyngeus), and persistent cough. A 2020 systematic review in Laryngoscope Investigative Otolaryngology found that more than 60% of LPR patients had no classic GERD heartburn. This diagnostic gap means LPR is frequently misdiagnosed as asthma, sinusitis, or allergies before the reflux connection is identified. Distinguishing the two matters because treatment protocols—particularly regarding acid suppression and dietary management—differ in meaningful ways between GERD and LPR.
- GERD: heartburn and esophageal symptoms dominate
- LPR: hoarseness, throat clearing, globus, postnasal drip—often no heartburn
- Misdiagnosis rate: frequently mistaken for sinusitis, asthma, or allergies
What lifestyle changes help reduce acid reaching the upper airway?
Several behavioral interventions carry the strongest evidence for reducing LPR symptom frequency. Elevating the head of the bed 6–8 inches using a wedge pillow or bed risers—not just extra pillows—reduces nocturnal reflux episodes because it uses gravity to keep gastric contents below the UES. The NIDDK recommends avoiding eating within 2–3 hours of lying down. Wearing loose-fitting clothing reduces intra-abdominal pressure. Tobacco use relaxes the LES and dramatically increases reflux frequency; cessation is one of the highest-yield interventions documented in clinical guidelines. Weight loss in overweight individuals reduces mechanical pressure on the LES. Smaller, more frequent meals reduce the volume of gastric content available for reflux compared to large single meals.
- Bed elevation: 6–8 inches using wedge or risers (not pillows alone)
- Meal timing: no food 2–3 hours before lying down
- Tobacco cessation: high-yield LES function improvement
- Clothing and meal size: reduce intra-abdominal pressure
What dietary changes reduce LPR symptoms?
Specific foods relax the lower esophageal sphincter or increase gastric acid production, worsening reflux. Identified triggers include caffeine, alcohol, chocolate, mint (peppermint and spearmint), citrus fruits, tomatoes, carbonated beverages, and high-fat foods. A 2017 study in JAMA Otolaryngology–Head and Neck Surgery found that a plant-based, Mediterranean-style diet reduced LPR symptoms comparably to proton pump inhibitor (PPI) therapy over 6 weeks. Alkaline foods—melons, oatmeal, bananas, ginger—are generally well-tolerated. Thickening liquids can reduce the speed at which refluxate reaches the UES. Keeping a food diary for 2–4 weeks helps identify individual triggers, since responses vary considerably between patients. Dietary changes typically take 4–8 weeks to show measurable impact on mucosal healing.
- Avoid: caffeine, alcohol, mint, citrus, carbonated beverages, high-fat foods
- Emphasize: alkaline and Mediterranean-pattern foods
- Food diary: 2–4 weeks identifies individual triggers
- Timeline: 4–8 weeks for mucosal improvement
What does the evidence say about acid-reducing treatments for LPR?
Proton pump inhibitors (PPIs) like omeprazole and lansoprazole are first-line pharmacological treatments for confirmed LPR, but evidence for their effectiveness specifically in LPR is weaker than for GERD. A 2022 meta-analysis in Alimentary Pharmacology & Therapeutics found PPIs improved LPR symptoms in 63% of patients versus 48% placebo response—a modest but statistically significant benefit. Alginate formulations (e.g., Gaviscon Advance) form a physical raft that prevents refluxate from reaching the pharynx and show benefit specifically for LPR in preliminary trials. Baclofen, a GABA-B agonist, reduces transient LES relaxations but is reserved for refractory cases due to side effects. H2 blockers (famotidine, ranitidine) provide less acid suppression than PPIs but may suit mild cases. All pharmacological approaches should be directed by a physician.
- PPIs (omeprazole, lansoprazole): first-line; 63% symptom response in meta-analysis
- Alginate raft therapy: addresses mechanical reflux reaching pharynx
- Baclofen: reduces LES relaxations; reserved for refractory LPR
- H2 blockers: useful for mild LPR under physician guidance
FAQ
Is LPR serious?
LPR is not immediately life-threatening but chronic, untreated reflux reaching the larynx and pharynx can cause long-term mucosal damage, increased risk of vocal cord granulomas, and—in rare cases—has been associated with laryngeal pathology. Anyone with persistent hoarseness lasting more than 2–3 weeks, swallowing difficulty, or unexplained throat symptoms should seek evaluation from an ENT physician. Early intervention reduces the risk of chronic changes.
Can acid really reach the ears?
Yes, via the Eustachian tube. The Eustachian tube connects the middle ear cavity to the nasopharynx; when LPR-related refluxate reaches the nasopharynx, pepsin and acid can travel into the tube and cause inflammation. A preliminary 2019 study in Otolaryngology–Head and Neck Surgery identified pepsin in middle ear fluid samples in a subset of LPR patients, supporting this pathway.
How long does it take for LPR to heal?
Mucosal tissue in the larynx and pharynx heals more slowly than esophageal tissue. Clinical guidelines suggest that consistent treatment—lifestyle changes plus appropriate pharmacotherapy if prescribed—typically takes 2–3 months to produce significant symptom reduction. Full mucosal healing in the larynx may take 6 months or longer in moderate-to-severe cases.
Is LPR the same as post-nasal drip?
Post-nasal drip is a symptom, not a diagnosis, and LPR is one of its leading causes. LPR-triggered post-nasal drip occurs because acid and pepsin irritate the mucosal lining of the nasopharynx, stimulating excess mucus secretion. Other causes of post-nasal drip—including allergic rhinitis, chronic sinusitis, and vasomotor rhinitis—require different management, which is why accurate diagnosis matters.
Should I see a doctor or can I manage LPR at home?
Lifestyle changes and dietary modification are appropriate first steps for mild, intermittent symptoms. However, LPR shares symptoms with more serious conditions including laryngeal pathology, esophageal motility disorders, and thyroid disease. If symptoms persist beyond 4–6 weeks of lifestyle modification, worsen, or include difficulty swallowing, weight loss, or blood in saliva or stool, a physician evaluation is necessary. A laryngoscopic exam can visualize laryngeal irritation patterns characteristic of LPR.
Does sleeping position affect LPR symptoms?
Yes. Sleeping on the left side reduces reflux frequency compared to the right side because stomach anatomy positions the gastroesophageal junction above the gastric body during left-lateral sleep. A small RCT published in The American Journal of Gastroenterology found significantly lower reflux episodes in left-side sleepers. Combining left-side positioning with head-of-bed elevation provides additive benefit for LPR patients.
Can stress worsen LPR?
Preliminary research suggests stress increases gastric acid production and may reduce LES tone, increasing reflux frequency. Psychological stress also amplifies visceral pain sensitivity, meaning patients may perceive reflux symptoms more intensely during stressful periods. Stress management approaches—including cognitive behavioral therapy (CBT) and mindfulness-based stress reduction (MBSR)—have directional evidence for improving functional GI symptoms, though their specific effect on LPR has not been well-studied in isolation.
—
For a comparison of digestive support supplements that may help with acid-related symptoms, see Supplement Buyers Lab.
Leave a Reply