
Stomach pain after every meal usually means digestion is triggering a repeatable pattern: stomach stretching, gas movement, acid reflux, food intolerance, constipation, or gut-brain sensitivity. The timing, location, stool changes, and food pattern matter more than one meal. Persistent, worsening, severe, or bloody symptoms need medical evaluation.
How did we evaluate post-meal stomach pain?
This article evaluated post-meal stomach pain by matching symptom timing, pain location, stool pattern, and food exposure against digestive physiology and clinical reference criteria. Government health sources, PubMed-indexed gastroenterology reviews, and NIDDK patient guidance received priority over anecdotes, supplement claims, social-media elimination diets, and single-person food rules. The review excluded commercial recommendations, disease labels without clinician confirmation, and claims that one food, ingredient, or routine explains every case. Evidence strength is separated from directional evidence: NIDDK symptom pages describe recognized clinical patterns, while mechanistic explanations such as visceral hypersensitivity and gut-brain signaling explain carefully why similar meals can produce different pain levels in different people. The limitation is practical: symptom patterns can guide safer next steps, but only medical evaluation can confirm conditions such as gallbladder disease, celiac disease, ulcers, or inflammatory bowel disease.
What is post-meal stomach pain and how does digestion trigger it?
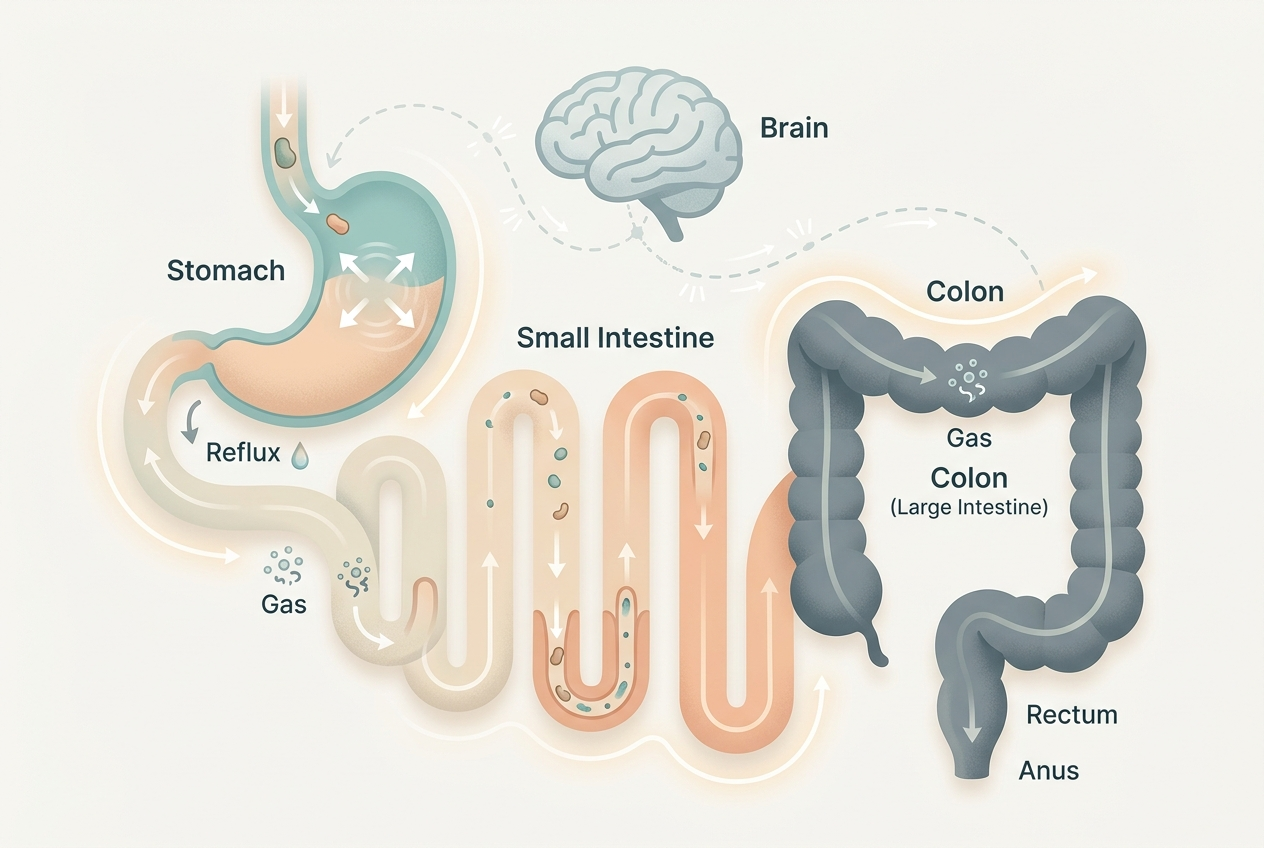
Post-meal stomach pain is abdominal discomfort that appears reliably after eating and fades, shifts, or worsens as food moves through the stomach, small intestine, and colon. Digestion triggers stomach stretching, acid secretion, bile release, pancreatic enzyme flow, intestinal gas movement, and the gastrocolic reflex. The gastrocolic reflex tells the colon to move after food enters the stomach, so lower-abdominal cramping can follow even when the meal itself is not harmful. Upper-abdominal burning, early fullness, nausea, or pressure can fit indigestion patterns; NIDDK describes dyspepsia as upper-abdominal discomfort that may include fullness, bloating, nausea, burping, or burning (NIDDK). Post-meal pain becomes more informative when timing is consistent: minutes suggests reflux, stretching, or anxiety-linked gut response, while one to four hours suggests fermentation, lactose exposure, constipation pressure, delayed intestinal movement, meal-size effects, or a strong colon reflex.
Which symptom patterns help separate common triggers?
Symptom pattern gives better clues than food blame alone. Burning behind the breastbone, sour taste, or throat irritation points toward reflux physiology, especially after large meals, alcohol, peppermint, chocolate, or lying down. Tight upper-abdominal pressure with early fullness points toward dyspepsia or slowed stomach emptying, but a clinician must confirm the cause. Bloating, audible gas, and cramping that improves after a bowel movement points toward gas handling, constipation, or IBS-type gut sensitivity; NIDDK lists abdominal pain related to bowel movements plus stool changes as core IBS symptoms (NIDDK). Pain plus diarrhea after milk, ice cream, whey, or soft cheese points toward lactose intolerance; NIDDK reports that lactose intolerance symptoms can include bloating, diarrhea, gas, nausea, and abdominal pain within hours after lactose exposure (NIDDK). Right-sided pain after fatty meals needs clinical review because gallbladder patterns can overlap with indigestion.
When should stomach pain after meals get medical attention?
Post-meal stomach pain needs medical attention when symptoms are severe, progressive, new after age 50, associated with vomiting, fever, fainting, black stool, blood in stool, unplanned weight loss, trouble swallowing, chest pain, or persistent right-upper-abdominal pain. These features do not prove a dangerous condition, but they raise the cost of guessing. Pain after every meal also deserves evaluation when it disrupts eating, sleep, work, hydration, or normal bowel patterns for more than a short stretch. A clinician can check medication effects, pregnancy status, gallbladder patterns, celiac disease risk, inflammatory markers, infection history, and alarm features before suggesting diet changes. Self-tracking helps that visit: record meal time, pain start time, pain location, stool form, gas, reflux, nausea, menstrual cycle timing, stress level, and medications. Clear records turn vague discomfort into a pattern that a primary care clinician or gastroenterologist can test.
What eating habits make after-meal pain more likely?
Eating habits can increase post-meal pain by increasing stomach pressure, fermentation load, or intestinal speed. Large meals stretch the stomach wall and increase reflux pressure. Fast eating increases swallowed air and reduces chewing, which can intensify belching and bloating. High-fat meals slow stomach emptying for some people, so fullness can last longer. Carbonated drinks add gas volume; NIDDK explains that gas in the digestive tract comes from swallowed air and bacterial fermentation of carbohydrates (NIDDK). Very high-FODMAP meals, including large servings of onion, garlic, wheat, beans, apples, and certain sweeteners, can increase fermentation in sensitive intestines. Skipping meals and then eating quickly can amplify the gastrocolic reflex. Habit changes are not a diagnosis, but smaller meals, slower eating, upright posture after meals, hydration, and consistent fiber intake can reduce mechanical triggers while the underlying pattern becomes clearer.
What does research say about gut-brain signaling and bloating?
Research supports a gut-brain model for recurring abdominal pain, especially when standard tests do not show structural disease. The enteric nervous system, vagus nerve, immune signaling, and microbiota-derived metabolites connect intestinal activity with pain perception. A Rome IV review in Gastroenterology describes centrally mediated gastrointestinal pain as pain generated or amplified by altered gut-brain processing rather than tissue injury alone (PubMed). This evidence is strong for the existence of gut-brain disorders, but it does not identify one universal cause for every person with post-meal pain. Bloating also has multiple mechanisms: gas volume, abdominal wall reflexes, constipation, visceral sensitivity, and carbohydrate fermentation can each contribute. That is why identical meals can feel normal on one day and painful on another. Sleep loss, stress, rapid eating, constipation, and menstrual-cycle changes can lower the discomfort threshold without making the food itself unsafe.
What should you track before changing your routine?
A two-week symptom log can identify patterns without turning meals into a guessing game. Track meal time, ingredients, portion size, eating speed, caffeine, alcohol, carbonated drinks, pain location, pain intensity from 0 to 10, symptom start time, symptom duration, stool form, gas, reflux, nausea, sleep, stress, and menstrual-cycle timing when relevant. The most useful pattern is repeatability: dairy plus symptoms within hours, large evening meals plus reflux, wheat-heavy meals plus bloating, or constipation plus lower-abdominal cramping. Avoid removing many food groups at once because broad restriction can hide the real trigger and reduce diet quality. Change one variable at a time for several days, such as portion size, meal speed, lactose exposure, carbonation, or late-night eating. If symptoms are frequent, severe, or worsening, bring the log to a clinician instead of escalating restriction alone.
For a detailed comparison of specific products and strains, see Bloating Every Afternoon? Compare Fiber, Probiotics, and Enzymes.
For a detailed comparison of specific products and strains, see Upper Middle Stomach Pain and Bloating: Options to Compare Before Guessing.
What questions do people ask about stomach pain after meals?
Is stomach pain after every meal normal?
No. Occasional discomfort can happen, but pain after every meal is a repeatable symptom pattern that deserves tracking and, if persistent, medical review.
Can bloating cause stomach pain after eating?
Yes. Gas, constipation, fermentation, and abdominal wall reflexes can stretch sensitive tissue and create cramping, pressure, or visible distension.
Does pain after eating mean a food intolerance?
Sometimes. Lactose, high-FODMAP carbohydrates, and large high-fat meals can trigger symptoms, but stress, reflux, constipation, and gut-brain sensitivity can mimic food reactions.
Should I stop eating the foods that hurt?
Start with a short symptom log before broad restriction. Remove one suspected trigger at a time only when the pattern repeats clearly.
When is post-meal pain urgent?
Severe pain, chest pain, fainting, fever, vomiting, black stool, blood in stool, trouble swallowing, or unplanned weight loss needs prompt medical attention.
Leave a Reply