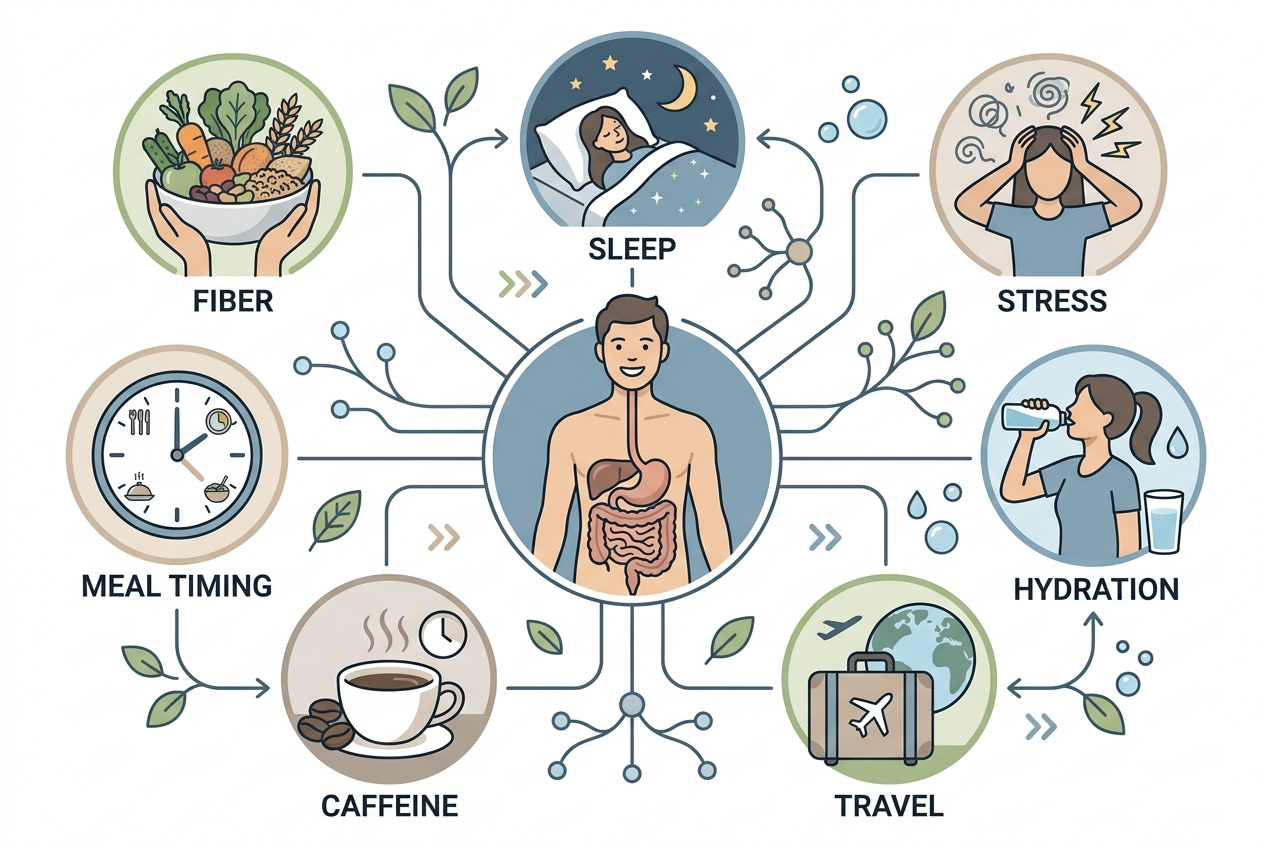
Digestion can feel different every week because gut motility, stool water, gas production, stress hormones, sleep timing, menstrual hormones, medications, alcohol, fiber intake, and meal composition change from week to week. The pattern usually is not random; it often reflects repeated inputs that are hard to notice without tracking them.
How did we evaluate weekly digestion changes?
We evaluated weekly digestion changes by separating normal digestive variability from patterns that deserve medical attention. Human physiology references from the National Institute of Diabetes and Digestive and Kidney Diseases, peer-reviewed gut microbiome research, and clinical diet literature received more weight than anecdotal explanations. We prioritized inputs people can observe directly, including meal timing, fiber amount, fluid intake, sleep, stress, alcohol, menstrual-cycle timing, and medication changes. We excluded product-specific advice because this cold-stage guide is educational, not a buying guide. The limitation is important: a symptom diary can clarify patterns, but it cannot rule out conditions that require evaluation. We also treated single bad days as weaker evidence than repeated clusters over time. Persistent pain, bleeding, unexplained weight loss, fever, nighttime diarrhea, repeated vomiting, or sudden severe change should be discussed with a clinician.
Why can digestion change from one week to the next?
Digestion changes weekly because the gastrointestinal tract responds to recent inputs rather than a fixed personal setting. The NIDDK explains that digestion moves food through the GI tract while nerves, hormones, muscles, enzymes, and gut bacteria coordinate breakdown and absorption. A week with later dinners, less sleep, more alcohol, less water, higher fat meals, or different fiber intake can change transit time and stool water. A week with more beans, onions, wheat, apples, protein bars, or sugar alcohols can change fermentation and gas. Stress can alter gut-brain signaling, and travel can shift meal timing, bathroom timing, and hydration. Menstrual-cycle changes can alter bowel patterns in some people. These drivers can overlap, which makes the result feel random. A seven-day view usually reveals more than a single bad day because patterns need repetition, not just memory.
What role does fiber play in week-to-week digestion?
Fiber changes digestion because different fibers hold water, add stool bulk, and feed colonic microbes at different rates. A review in Nutrients describes dietary fiber as a broad category that includes soluble, insoluble, viscous, and fermentable fibers, not one single substance. Soluble fibers such as psyllium can hold water and support stool form, while highly fermentable fibers such as inulin can increase gas when intake rises quickly. Insoluble fibers from wheat bran or vegetable skins can increase stool bulk, but tolerance varies by person and meal pattern. A low-fiber weekday followed by a high-fiber weekend can create a visible swing in stool form. The useful question is not “Is fiber good?” The useful question is “Which fiber changed, how much changed, how quickly did it change, and what else changed that day or weekend?”
How do sleep and stress affect digestion?
Sleep and stress affect digestion through the gut-brain axis, autonomic nervous system, and daily circadian timing. A review in Frontiers in Psychiatry describes bidirectional communication between the gut microbiota and central nervous system, although human responses vary and causality is not always simple. Short sleep can change meal timing, caffeine intake, appetite, and physical activity the next day. Psychological stress can change gut motility, visceral sensitivity, and bathroom routines for some people. Circadian disruption from late meals or shift work can make the same food feel different at a different time. These effects do not mean symptoms are imaginary. They mean the nervous system and digestive system share control loops. Tracking bedtime, wake time, caffeine, and stress alongside meals often explains swings that food lists miss, especially during busy weeks or travel periods.
Why can the same meal feel fine once and uncomfortable later?
The same meal can feel different because context changes the digestive load. A burrito eaten after a high-fiber breakfast, two coffees, poor sleep, and a stressful commute is not the same digestive event as the same burrito eaten after a normal night and a light lunch. Fat slows gastric emptying, fiber changes stool water and fermentation, and large portions stretch the stomach more than smaller portions. FODMAP-rich ingredients such as onion, garlic, wheat, beans, milk, apples, and certain sweeteners can ferment differently depending on dose and recent intake. Monash University researchers who developed the low-FODMAP approach emphasize that FODMAP tolerance is dose-dependent rather than all-or-nothing. The lesson is practical: repeated discomfort after the same food matters, but one uncomfortable meal rarely identifies the full trigger. Dose, timing, and the previous 24 hours matter more.
What should you track before assuming the problem is random?
Track timing, stool pattern, meal composition, hydration, sleep, stress, medications, alcohol, caffeine, exercise, and menstrual-cycle timing before assuming digestion is random. The Bristol Stool Form Scale gives a simple shared language for stool form, and a clinical review in Journal of Neurogastroenterology and Motility describes stool form as a useful proxy for intestinal transit time. A useful diary does not need calorie math. It needs consistent fields: wake time, first meal, fiber-heavy foods, dairy, high-fat meals, unusual sweeteners, bowel movements, pain, bloating, and stress level. Record the data for 10 to 14 days, then look for clusters across meals, sleep, and bowel timing. One clue rarely explains everything. Repeated combinations usually explain more than isolated foods, especially when weekends, travel, or stressful workdays differ from weekdays.
When should changing digestion be checked by a clinician?
Changing digestion should be checked when the pattern is severe, persistent, sudden, or paired with red-flag symptoms. Educational tracking is reasonable for mild, short-term swings, but it should not delay care for blood in stool, black stool, unexplained weight loss, fever, dehydration, persistent vomiting, nighttime diarrhea, anemia, new symptoms after age 50, or severe localized pain. The NIDDK notes that many digestive symptoms can have multiple causes, which is why context and duration matter. Medication changes, recent antibiotics, pregnancy, immune suppression, recent travel illness, and family history of gastrointestinal disease also change the risk calculation. A clinician can decide whether labs, stool tests, imaging, endoscopy, dietitian referral, or medication review is appropriate. A diary helps that visit because it turns vague timing into usable information and reduces guesswork during care decisions.
What questions do people ask about changing digestion?
Can normal digestion vary every week?
Yes. Normal digestion can vary with fiber amount, fluid intake, sleep timing, travel, stress, menstrual-cycle timing, alcohol, caffeine, and meal size. The key distinction is whether the variation is mild and explainable or severe, persistent, and worsening.
Does bloating always mean a specific food is bad for me?
No. Bloating can reflect portion size, fermentation, swallowed air, constipation, stress, menstrual-cycle timing, or a high-FODMAP load. A repeated pattern after the same food is more useful than one uncomfortable meal.
How long should I track digestion?
Track for 10 to 14 days if symptoms are mild and stable. That window usually covers weekdays, weekends, sleep differences, social meals, and stress changes. Seek care sooner for red-flag symptoms.
Can stress really change stool pattern?
Yes. Stress can affect gut motility, visceral sensitivity, appetite, caffeine intake, and bathroom timing. That does not make symptoms imaginary; it means the gut and nervous system communicate continuously.
Why does travel change digestion?
Travel changes meal timing, hydration, movement, sleep, bathroom access, alcohol intake, and food choices. Those changes can alter transit time and stool water even when no single travel food is the cause.
Should I cut out foods immediately?
Avoid cutting out many foods at once unless a clinician or dietitian recommends it. Broad restriction can obscure patterns and make eating harder. A better first step is tracking repeated dose-and-timing relationships.
For a detailed comparison of specific products and strains, see Why Digestive Relief Feels Temporary and What to Compare Next.
What is the bottom line?
Weekly digestion changes usually have a pattern, even when the pattern is not obvious. Meal timing, fiber type, fluid intake, sleep, stress, alcohol, caffeine, menstrual-cycle timing, travel, and medications can all change motility, stool water, and gas production. Start with a simple two-week diary before blaming one food or one supplement. Compare weekdays with weekends, early dinners with late dinners, high-fiber days with low-fiber days, and rested mornings with short-sleep mornings. If symptoms are severe, persistent, sudden, or paired with red flags, skip the self-experiment and get medical guidance. If the pattern points toward supplement comparison later, a separate buying guide can help compare options without mixing education and product decisions. The main goal is to replace “random” with a clearer set of repeatable clues that someone can actually act on confidently.
Leave a Reply