Mild stomach discomfort and bloating after a bowel movement can happen when stool movement, gas movement, rectal sensitivity, constipation, or pelvic-floor coordination changes how the gut feels after emptying. It is usually a pattern to track, not a diagnosis. Severe, new, persistent, or worsening symptoms need medical evaluation.
How did we evaluate bloating after a bowel movement?
We evaluated post-bowel-movement bloating by matching symptom timing to common digestive mechanisms: stool retention, gas transit, visceral sensitivity, pelvic-floor coordination, and bowel-habit changes. We prioritized NIDDK, MedlinePlus, NCBI Bookshelf, PubMed-indexed Rome IV discussions, and peer-reviewed reviews over anecdotal forum explanations, product-first claims, and social-media diagnosis language. We excluded product-first explanations because this question asks what the pattern may mean before anyone compares remedies, and we weighted tracking steps higher than one-size-fits-all advice. The main limitation is that symptom timing cannot identify one cause by itself; discomfort after a bowel movement can overlap with constipation, diarrhea, IBS-pattern symptoms, diet changes, medication effects, anxiety physiology, hemorrhoids, fissures, pelvic-floor tension, or unrelated abdominal problems. We also separated mild recurring patterns from red-flag patterns because those two groups need different next steps and different clinical urgency levels overall.
Why can bloating happen after you poop?
Bloating after a bowel movement can happen because the bowel movement changes pressure, gas position, and sensory signaling inside the colon and rectum. A person may empty some stool but still retain gas or stool higher in the colon. The rectum may also feel irritated after straining, urgency, diarrhea, or repeated wiping. In functional bowel disorders, normal stretch can feel stronger than expected because the gut-brain axis processes internal signals more intensely. A review in PMC describes visceral hypersensitivity as an important mechanism in irritable bowel syndrome, especially for pain and bloating perception (PMC). That does not mean every post-poop symptom is IBS. It means timing, stool form, straining, urgency, food pattern, bathroom duration, medication changes, and red flags matter more than one isolated episode. A single mild episode often tells less than a repeated pattern across similar meals and bowel movements.
What does constipation have to do with after-poop bloating?
Constipation can cause bloating after a bowel movement when stool remains in the colon or evacuation feels incomplete. MedlinePlus describes constipation as fewer than three bowel movements per week, hard or dry stool, or painful passage in many cases (MedlinePlus). NIDDK advises medical care when constipation persists despite self-care or appears with rectal bleeding, blood in stool, continual abdominal pain, or other concerning signs (NIDDK). A person can poop daily and still strain, pass small hard pieces, or feel unfinished. That pattern can leave gas trapped behind stool, make the abdomen feel distended, and create discomfort after the bathroom. Tracking Bristol stool type, straining, time on the toilet, urgency, and the sense of complete emptying gives more useful information than tracking frequency alone. The key question is not just “Did I go?” but “Was emptying easy and complete?”
Could pelvic-floor coordination be involved?
Pelvic-floor coordination can matter when the muscles that should relax during a bowel movement tighten, do not fully relax, or require straining to empty. NCBI Bookshelf notes that pelvic-floor dysfunction can involve incomplete evacuation, prolonged straining, or pressure during defecation (NCBI Bookshelf). This pattern can make someone feel bloated or uncomfortable after going because the rectum and lower bowel remain irritated or not fully emptied. Clues include long bathroom sessions, repeated trips, narrow stool, needing to change position, breath-holding, or feeling like more stool remains. This is not something to self-diagnose from one symptom. A clinician, gastroenterologist, or pelvic-floor physical therapist can evaluate coordination problems when the pattern is persistent, especially when ordinary fiber, water, walking, and routine changes do not help. The practical clue is effort: easy bowel movements usually point away from coordination trouble.
How can you track the pattern before guessing?
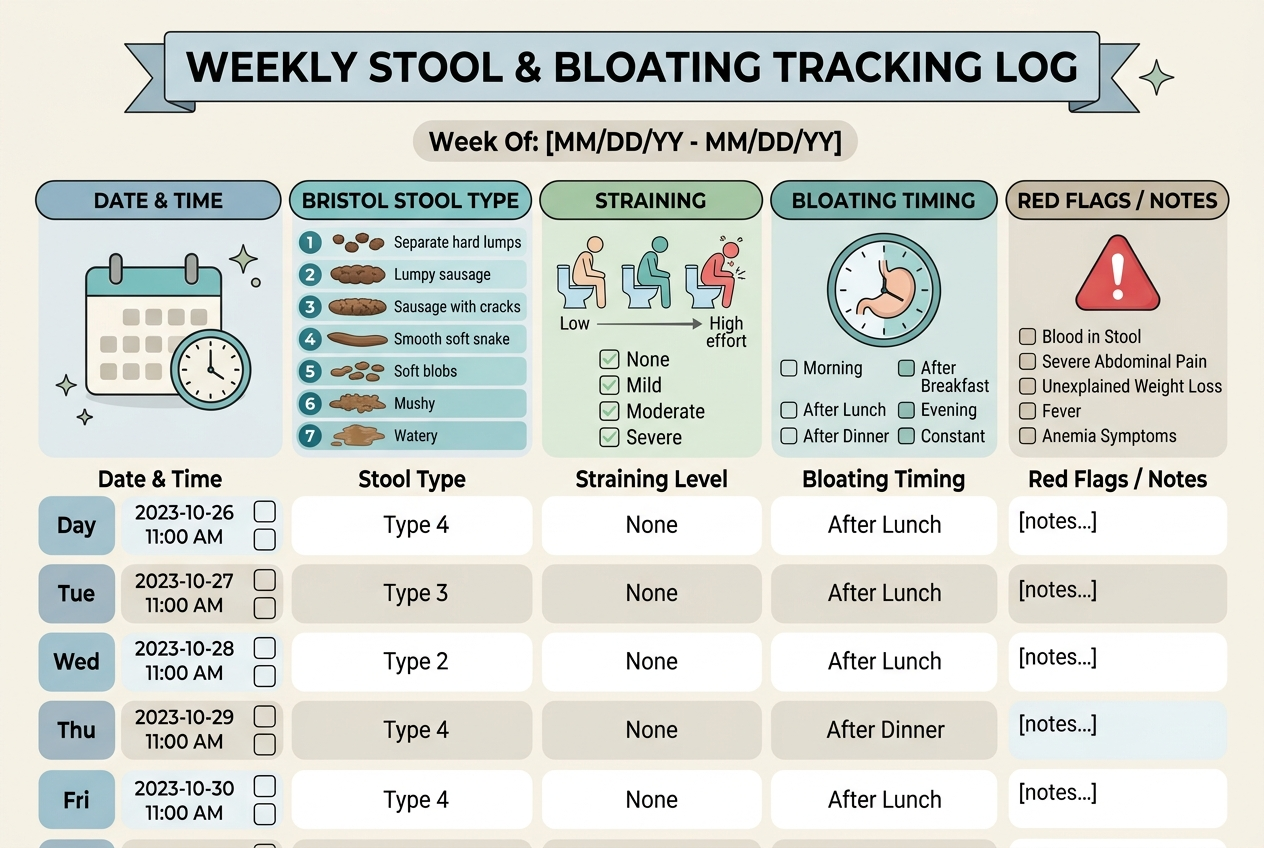
Track the pattern for one to two weeks with four data points: stool form, straining, timing of bloating, and food or drink triggers. The Bristol Stool Form Scale can help describe stool texture more precisely than “normal” or “weird.” Note whether bloating begins before the bowel movement, immediately after, or one to three hours later. Also note carbonated drinks, large meals, dairy, beans, onions, wheat, sugar alcohols, high-fat meals, caffeine, stress, new medications, and menstrual-cycle timing when relevant. Rome IV discussions define IBS around recurrent abdominal pain related to defecation and bowel-habit changes, but clinical interpretation belongs with a healthcare professional (Rome IV review). A log helps separate occasional gas movement from constipation, diarrhea, urgency, incomplete evacuation, or escalating symptoms. It also gives a clinician concrete details if the pattern continues beyond basic routine changes.
When should after-poop bloating be checked?
After-poop bloating should be checked promptly when it is severe, progressive, new after age 50, associated with fever, vomiting, blood, black stool, unexplained weight loss, anemia, persistent diarrhea, nighttime symptoms, or ongoing abdominal pain. It should also be checked when constipation does not improve with basic self-care or when bowel habits change suddenly and stay changed. These red flags do not prove a serious condition, but they move the question out of self-tracking territory. Mild discomfort that comes and goes with stool form, meal size, or straining can often be logged first. Persistent patterns deserve a clinician because stool retention, pelvic-floor dysfunction, IBS, medication effects, infections, inflammatory conditions, and structural problems can overlap. The goal is not alarm; the goal is not missing the pattern that needs care. New symptoms after antibiotics, surgery, travel, or major medication changes deserve extra caution.
What questions do people ask about bloating after bowel movements?
Is it normal to feel bloated after pooping?
Occasional bloating after a bowel movement can happen, especially with gas, constipation, straining, or large meals. It is worth tracking when it repeats, worsens, or appears with pain or bowel-habit changes.
Can incomplete emptying cause bloating?
Yes, incomplete evacuation can leave stool or gas behind and create pressure after the bathroom. Clues include straining, multiple trips, hard stool, or feeling unfinished.
Can IBS cause discomfort after bowel movements?
IBS-pattern symptoms can include abdominal pain related to defecation and altered bowel habits. Only a clinician can interpret whether a recurring pattern fits IBS or another condition.
Does diarrhea cause after-poop bloating?
Diarrhea can irritate the rectum and change gas movement, so bloating or discomfort can appear afterward. Persistent diarrhea, dehydration, fever, blood, or nighttime symptoms should be checked.
Should I take fiber for this pattern?
Fiber may help constipation-leaning patterns, but sudden increases can worsen gas and bloating. Increase fiber gradually and track stool form, water intake, and symptoms.
What should I write down for a doctor?
Write down stool frequency, Bristol stool type, straining, pain location, bloating timing, blood, weight change, medications, supplements, and food patterns. A clear log is more useful than a vague “my digestion is off.”
What is the practical next step?
For mild recurring bloating after a bowel movement, track stool form, straining, timing, and incomplete-emptying sensations for one to two weeks. Improve basics first: steady fluids, regular bathroom time, gradual fiber, gentle walking, and less straining. Avoid changing several variables at once because that makes the pattern harder to interpret. If stool is hard, start with constipation basics. If stool is loose or urgent, track food timing, caffeine, stress, and recent illness. If emptying feels incomplete despite regular bowel movements, ask about pelvic-floor coordination rather than assuming the issue is only diet. Seek medical care sooner if symptoms are severe, new, persistent, worsening, or paired with red flags. A clear symptom log makes that visit faster and more useful because it shows timing, severity, and stool pattern instead of relying on memory alone later.
Leave a Reply