Lactose-free milk can still cause digestive symptoms because it removes or breaks down lactose, but it does not remove milk proteins, fat, additives, serving size effects, or reflux triggers. If lactose-free milk still causes bloating, nausea, diarrhea, or reflux, the pattern may involve something besides lactose alone.
How did we evaluate why lactose-free milk can still cause symptoms?
We evaluated lactose-free milk symptoms by separating lactose malabsorption, milk protein reactions, fat tolerance, reflux mechanics, serving size, and food-additive tolerance. NIDDK and MedlinePlus references received more weight than anecdotal reports because they define lactose intolerance, symptom timing, and differences from milk allergy. We excluded claims that assume one home reaction proves one cause, because digestive symptom patterns overlap. We also prioritized practical tracking steps over supplement or product recommendations because this is a cold educational question. Repeated timing, portion size, and symptom type received more weight than one isolated episode. We treated brand switches, fat changes, coffee use, and bedtime drinking as confounders because each can change the result. The main limitation is that a home food log can identify patterns, but it cannot confirm allergy, malabsorption, reflux, IBS, or another digestive condition by itself.
Why can lactose-free milk still bother your stomach?
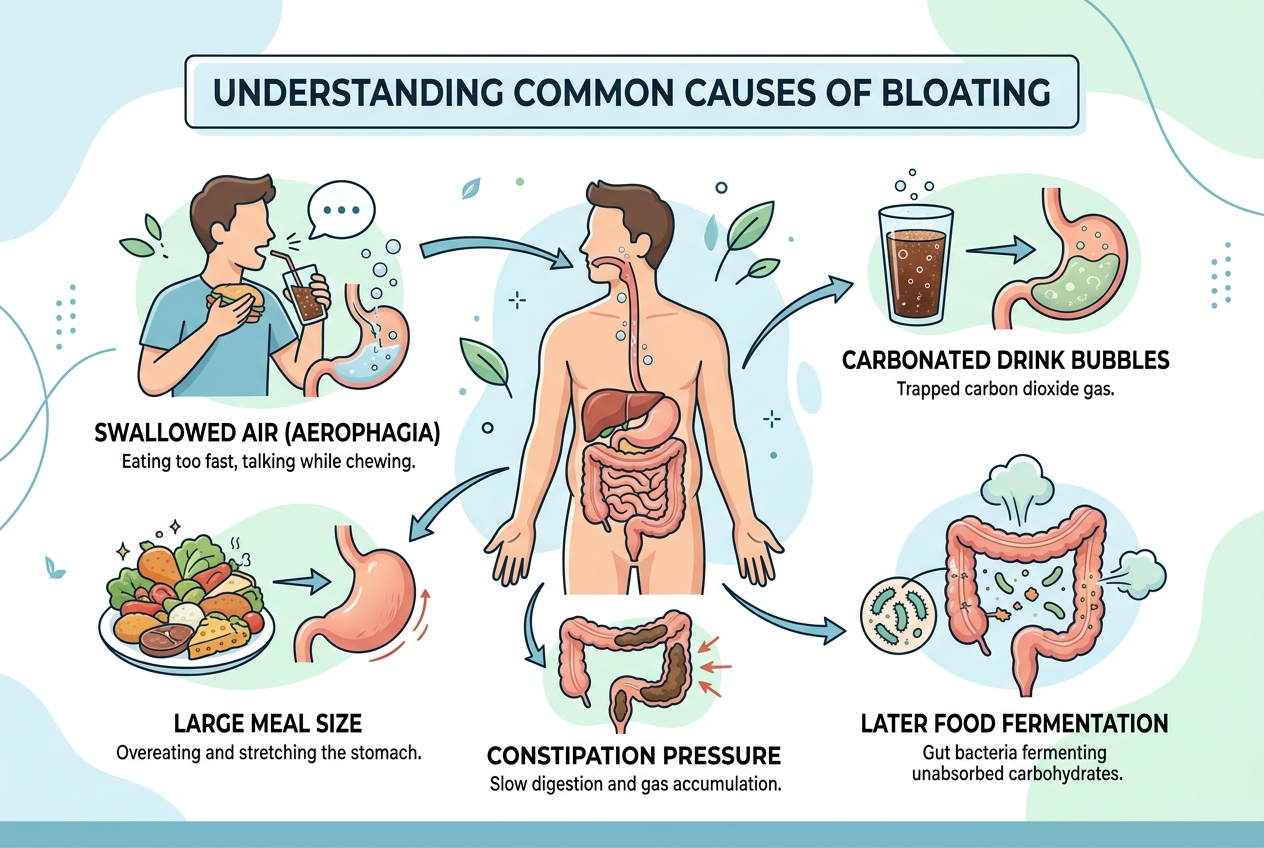
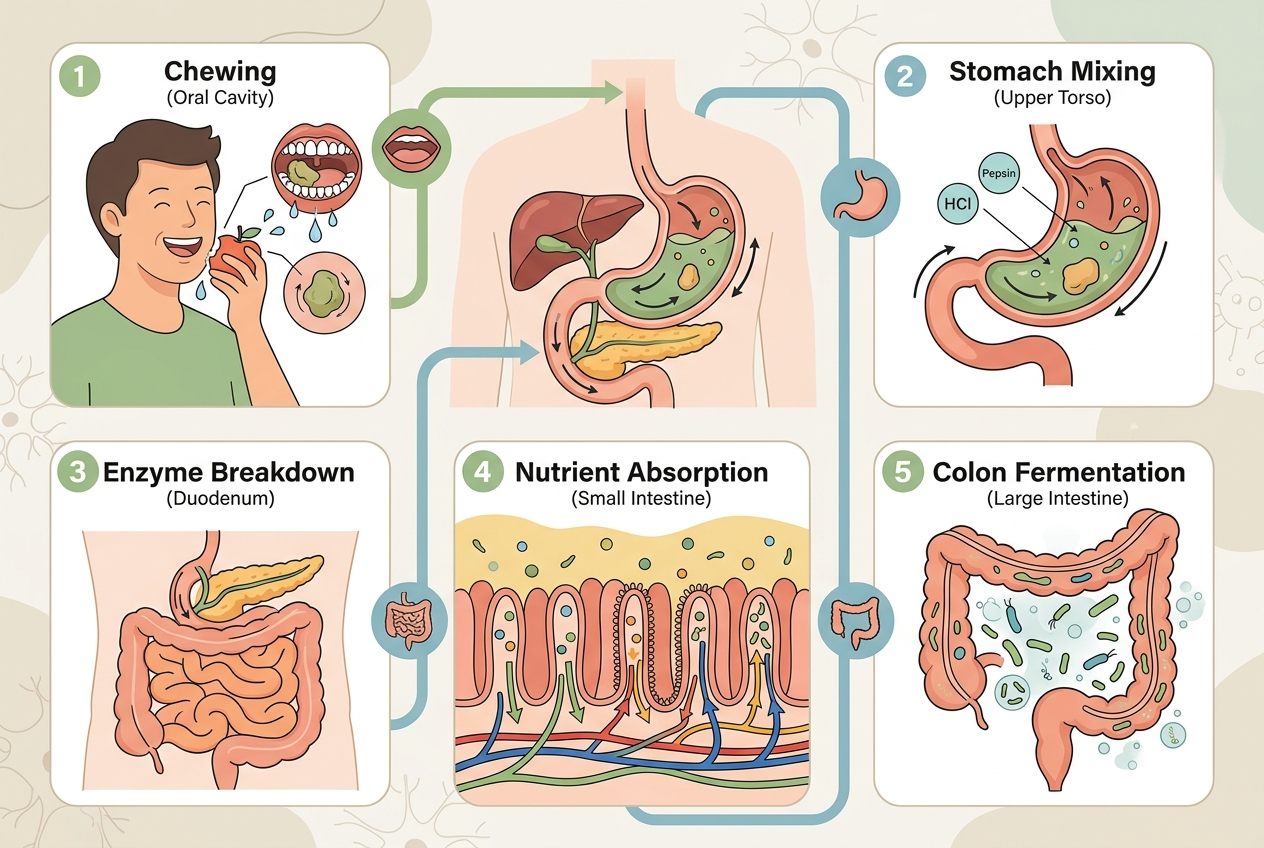
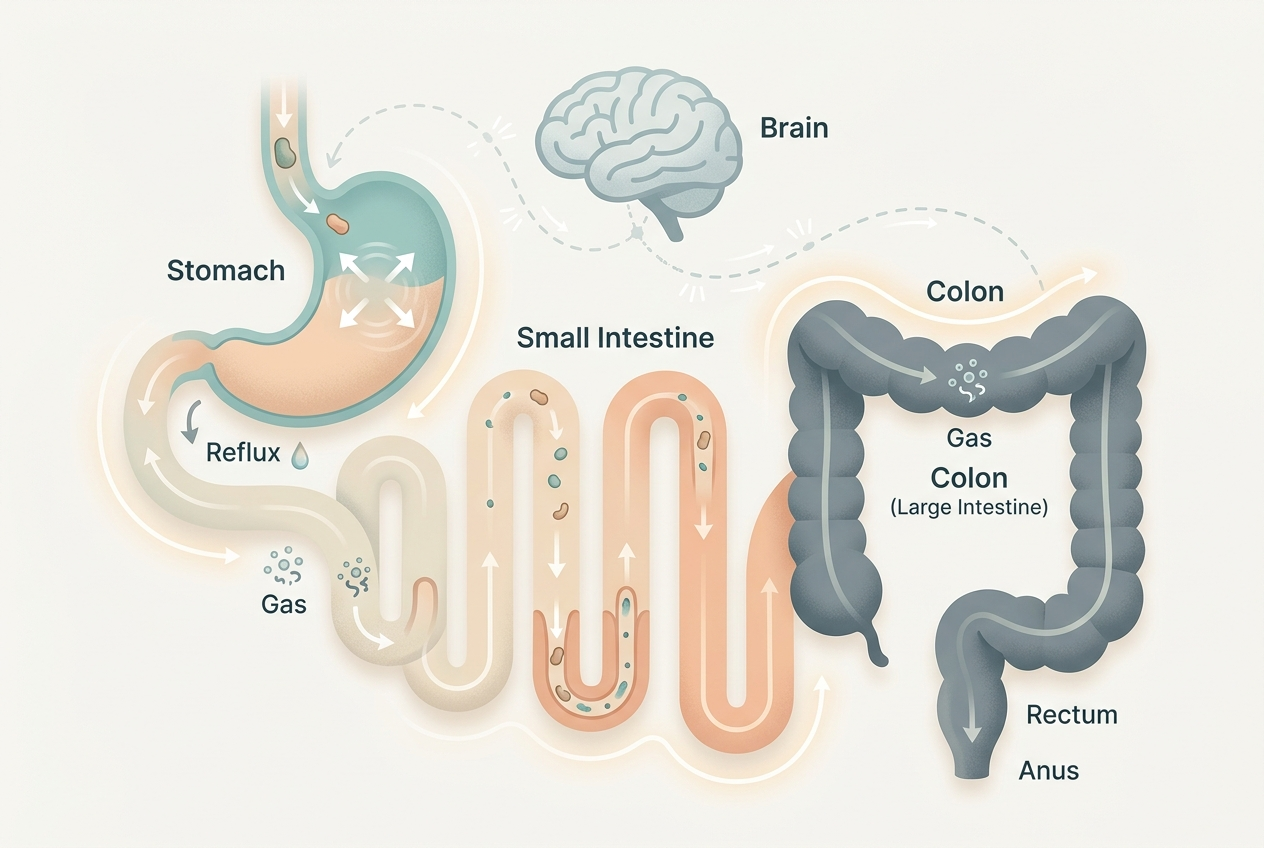
Lactose-free milk changes lactose, not the entire milk matrix. Lactase-treated milk breaks lactose into glucose and galactose, but the drink still contains dairy proteins, fat, minerals, and the same liquid volume. NIDDK explains that lactose intolerance symptoms occur when undigested lactose reaches the colon and bacteria create gas and fluid, causing bloating, diarrhea, gas, nausea, abdominal pain, and rumbling within a few hours through its lactose intolerance overview. If lactose-free milk causes the same symptoms, the issue may be residual lactose sensitivity, milk protein sensitivity, high serving volume, high-fat dairy, reflux overlap, sweetener tolerance, or an unrelated flare. Coffee, cereal, protein powder, and bedtime timing can also confuse the pattern. The clue is repeatability: the same amount, same brand, same timing, and same symptom window tell more than one bad glass.
How is lactose intolerance different from milk allergy or reflux?
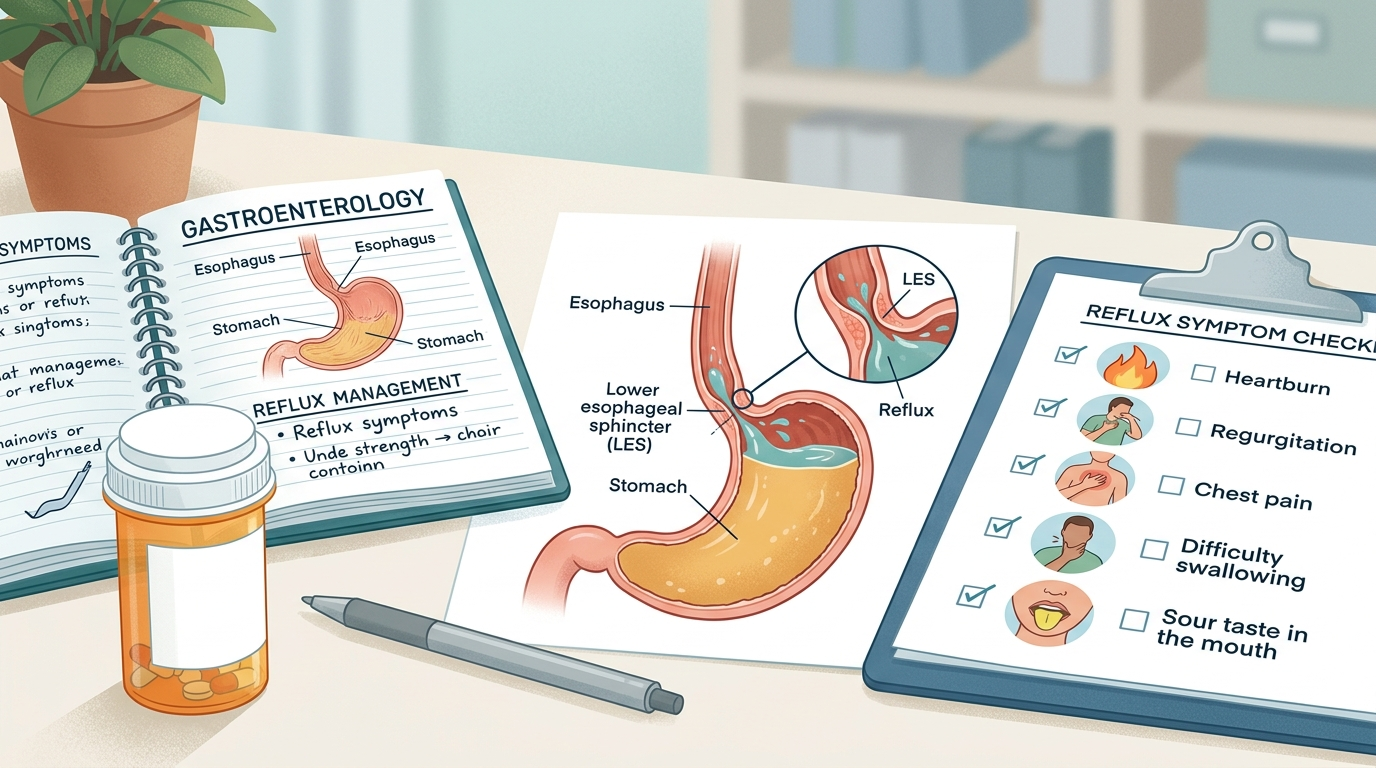
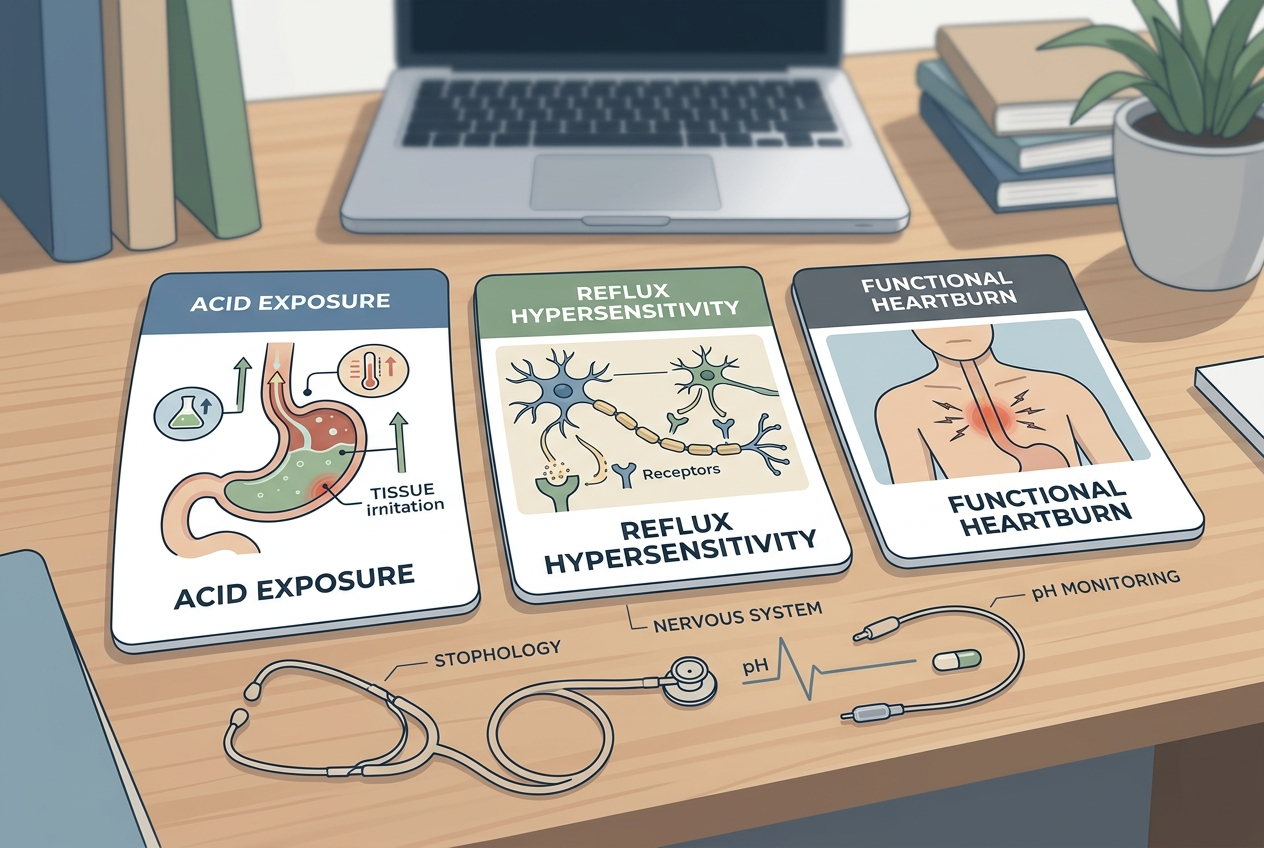
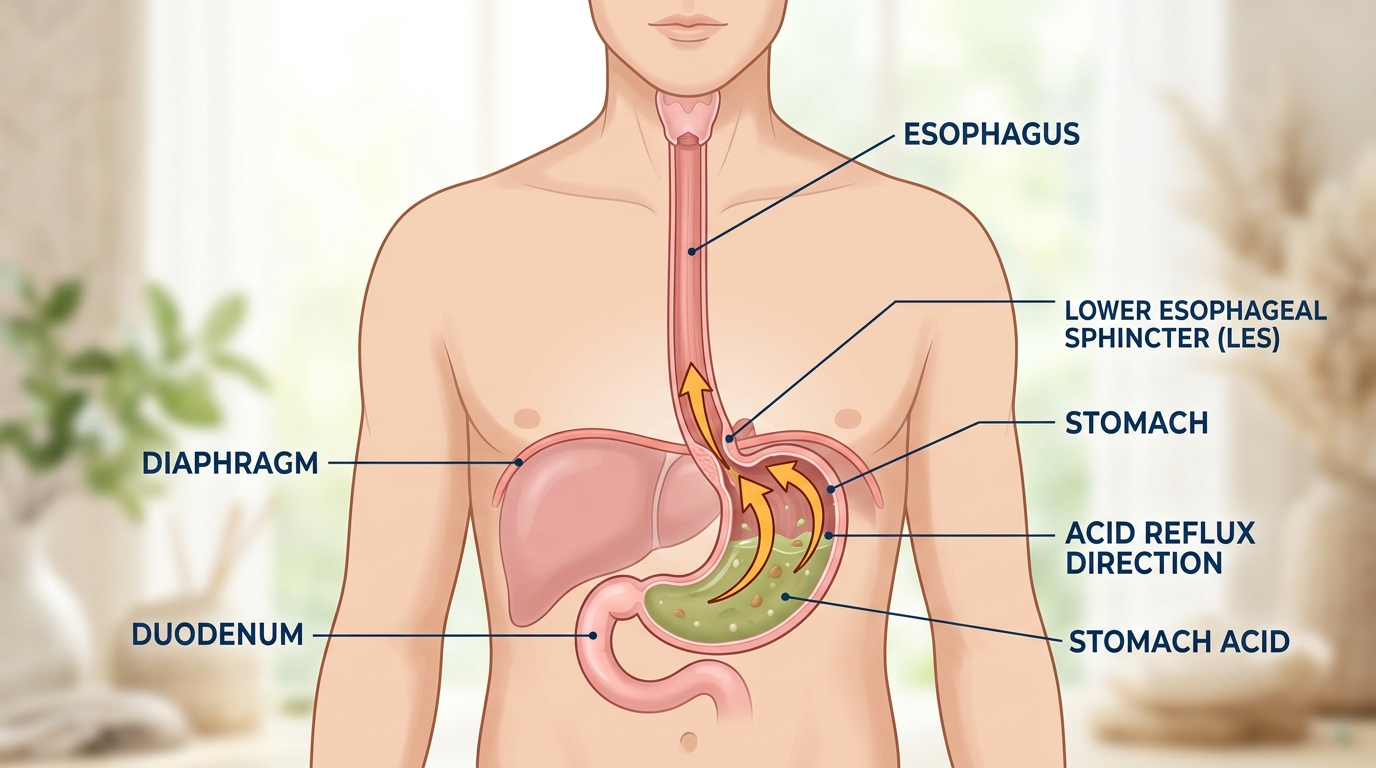
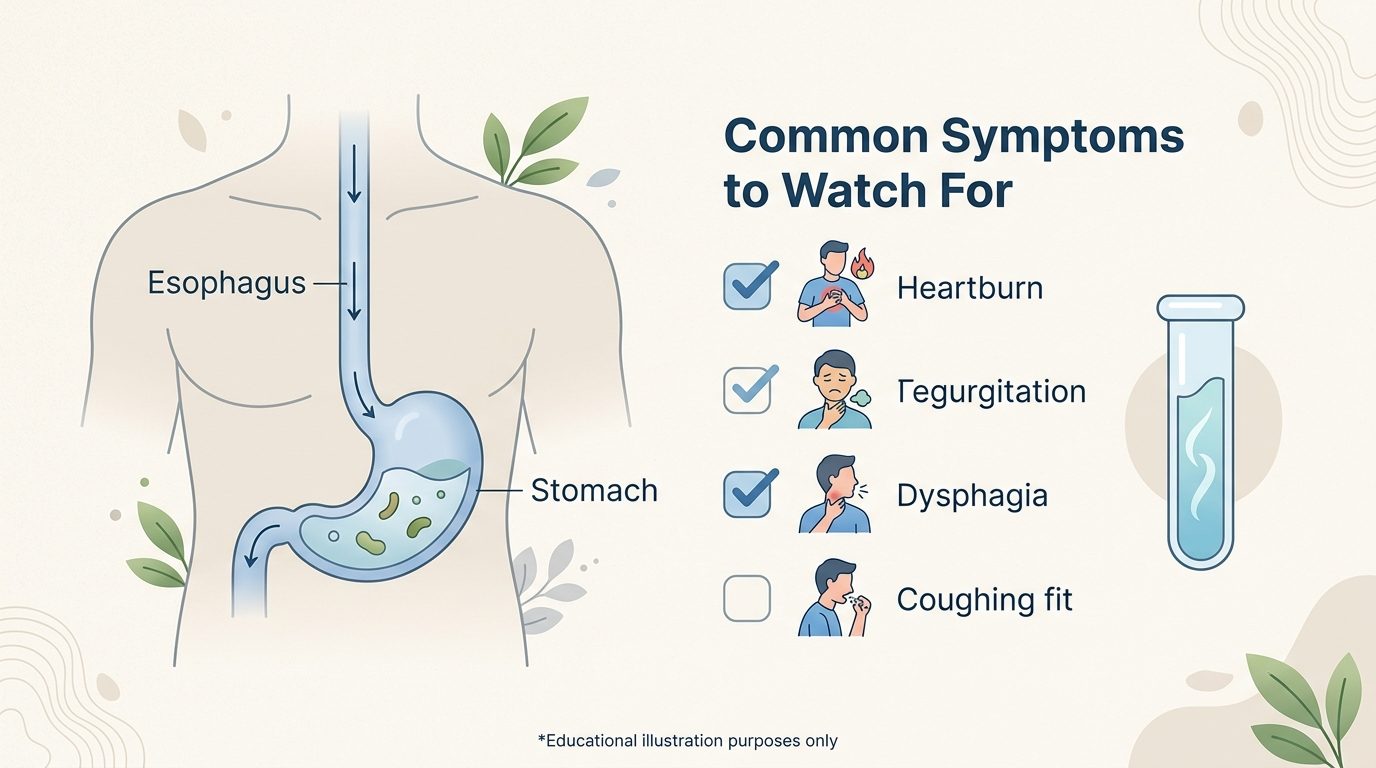
Lactose intolerance involves difficulty digesting lactose, while milk allergy involves the immune system reacting to milk proteins. NIDDK states that lactose intolerance and milk allergy have different causes, and a serious milk allergy reaction can be life threatening. Reflux is a separate pattern in which stomach contents move upward, often shaped by meal volume, fat content, timing, and body position. That means one person can react to regular milk from lactose, another can react to lactose-free milk from dairy protein, and another can feel reflux after any large evening drink. Symptom type helps sorting. Lower-abdominal gas, rumbling, diarrhea, and cramps after dairy fit lactose malabsorption more closely. Burning, regurgitation, throat irritation, or symptoms after lying down fit reflux mechanics more closely. Skin, breathing, mouth, or throat symptoms point away from simple lactose intolerance. Hives, swelling, wheezing, or rapid systemic symptoms need urgent medical attention.
What should you track before assuming lactose-free milk is the problem?
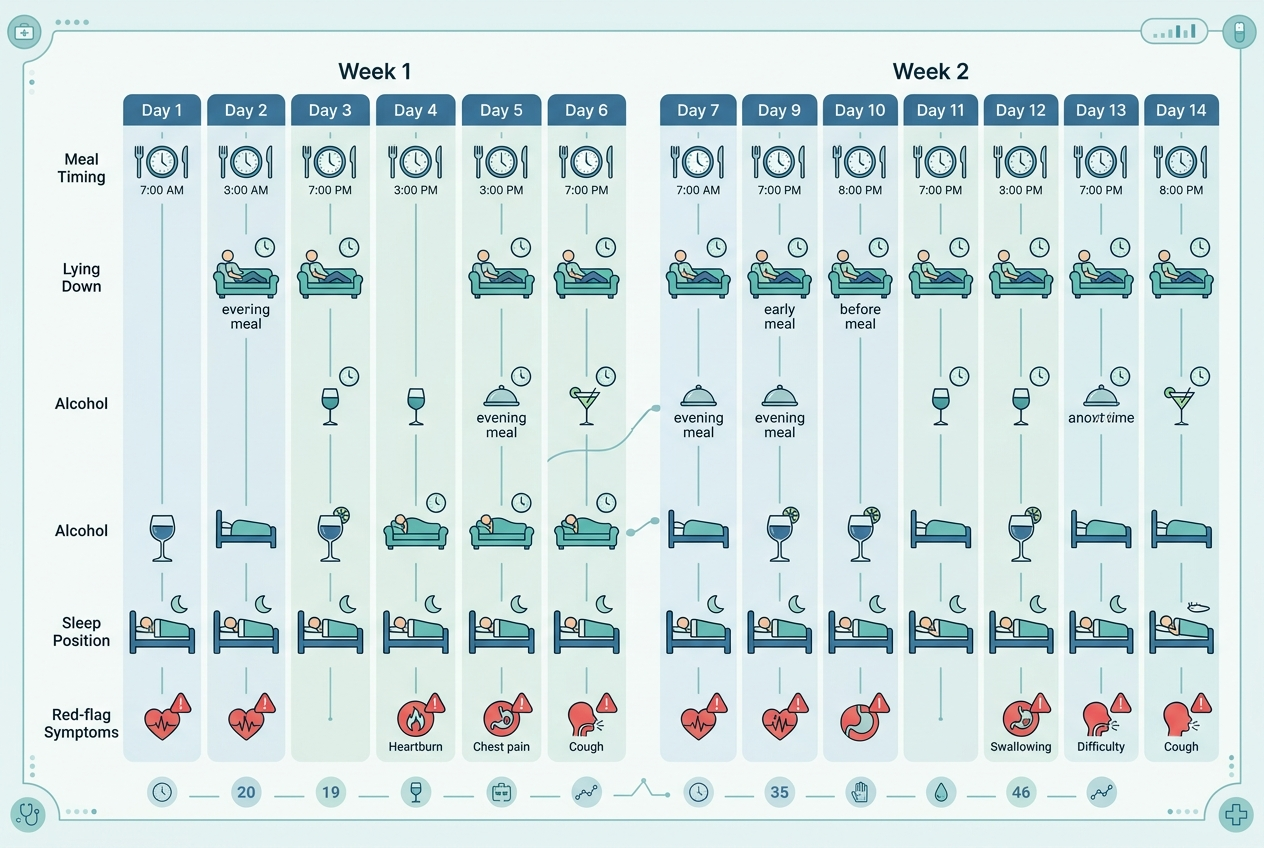
Track the brand, serving size, fat level, temperature, timing, added ingredients, and what else was eaten within four hours. A small lactose-free milk serving with a meal is a different test than a large cold glass before bed. NIDDK notes that clinicians may use medical history, family history, diet history, and tests when diagnosing lactose intolerance through its diagnosis guidance. A useful home log records symptom onset, symptom type, severity, bowel changes, reflux sensations, and repeat exposures. Compare lactose-free cow’s milk against regular milk, A2 milk, yogurt, hard cheese, soy milk, oat milk, and water with similar meal timing. If every dairy form causes symptoms, dairy protein or fat may be relevant. If only milk causes symptoms, serving size, speed, or liquid volume may matter.
What milk alternatives are worth comparing?
Milk alternatives should be compared by protein, fat, fiber, fortification, sweeteners, and tolerance rather than by marketing category. Unsweetened soy milk usually provides more protein than almond, oat, or rice beverages. Oat milk can contain more carbohydrate and gums, which may matter for people sensitive to fermentable carbohydrates or thickeners. Almond milk is often lower in protein unless fortified or blended. Lactose-free cow’s milk keeps dairy protein and nutrients but changes lactose. Calcium and vitamin D fortification matter if dairy is being removed long term. Coconut milk can be higher in saturated fat, which may matter for reflux-prone drink timing. A practical comparison uses one unsweetened option at a time for several days while keeping breakfast, coffee, and bedtime timing similar. Switching five variables at once makes the result impossible to read. The best alternative is the one that gives consistent tolerance and fits the person’s nutrition needs.
When should lactose-free milk symptoms be checked?
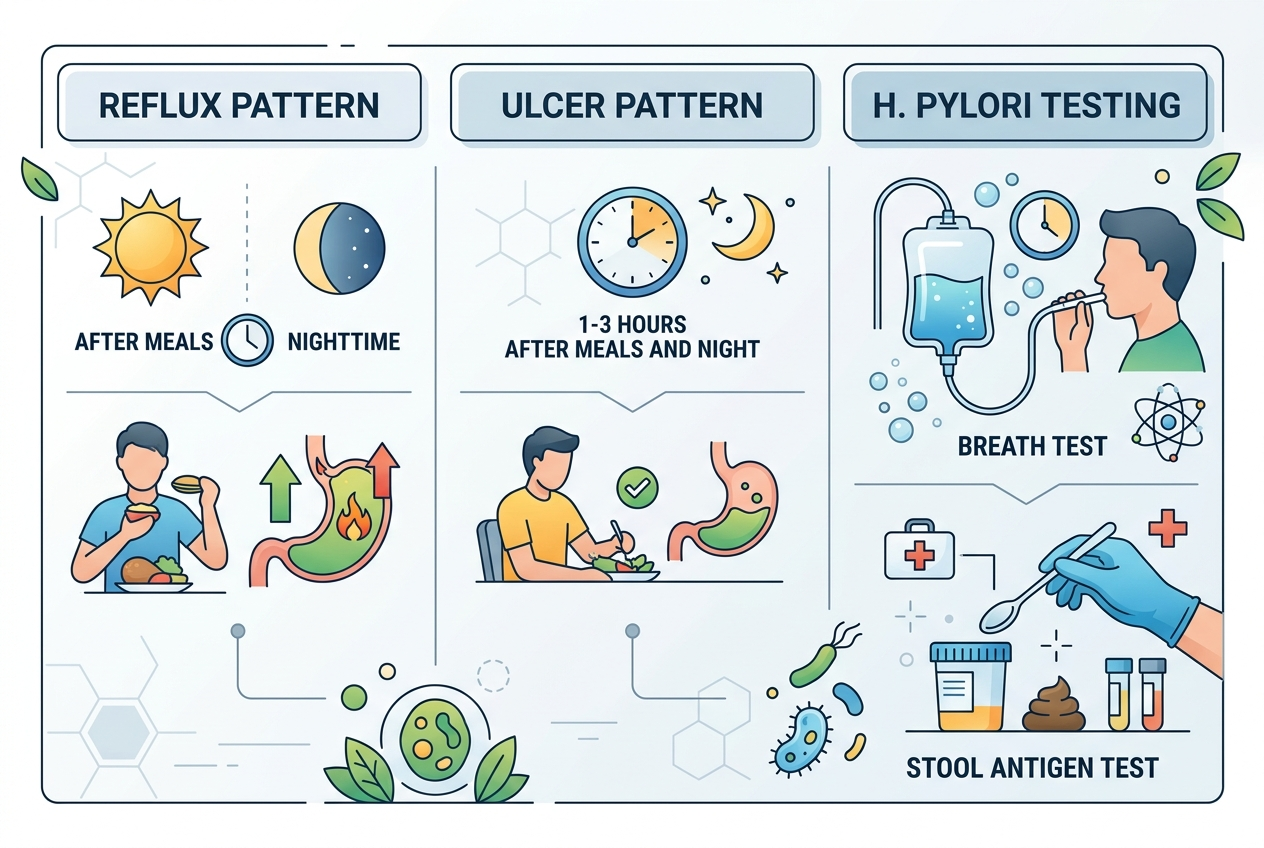
Symptoms should be checked when they are persistent, severe, escalating, or paired with red flags such as weight loss, blood in stool, repeated vomiting, trouble swallowing, dehydration, fever, anemia, or nighttime symptoms that wake you. Lactose-free milk reactions can be simple intolerance patterns, but they can also overlap with reflux, IBS, food allergy, celiac disease, inflammatory bowel disease, gallbladder issues, or medication effects. Mayo Clinic notes that lactose intolerance can occur when the small intestine produces too little lactase, and secondary lactose intolerance can follow illness, injury, or small-intestine conditions in its lactose intolerance overview. A clinician can decide whether history, elimination and re-challenge, breath testing, allergy evaluation, or reflux evaluation fits the pattern. The safest rule is simple: repeated symptoms deserve pattern tracking, and red flags deserve medical care.
What questions do people ask about lactose-free milk symptoms?
Does lactose-free milk still have lactose?
It can contain very small residual amounts depending on product and processing. Most people with lactose intolerance tolerate lactose-reduced products better, but individual sensitivity and serving size still matter.
Can milk protein cause symptoms if lactose is removed?
Yes. Lactose-free milk still contains dairy proteins, including casein and whey. Milk protein reactions are different from lactose malabsorption and should be evaluated carefully if symptoms suggest allergy.
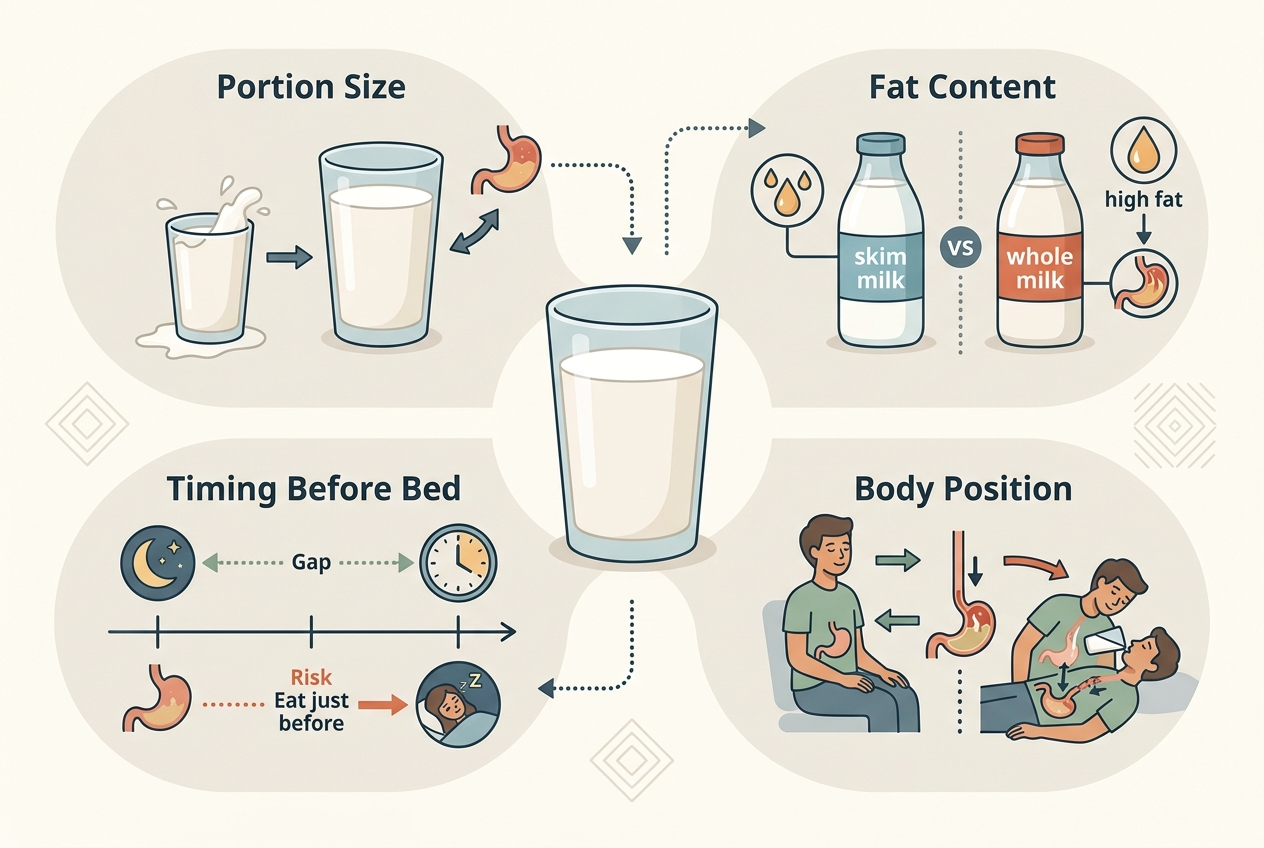
Can lactose-free milk trigger reflux?
It can contribute to reflux-like symptoms if volume, fat content, timing, or lying down after drinking are the main drivers. Removing lactose does not change those reflux mechanics.
Is oat milk always easier to digest?
No. Oat milk removes dairy proteins and lactose, but it may contain gums, oils, added sugars, or fermentable carbohydrates that bother some people.
Should I avoid all dairy if lactose-free milk bothers me?
Not automatically. Some people tolerate yogurt, kefir, hard cheese, or smaller portions better than milk because the food matrix, lactose amount, and serving size differ.
What is the cleanest home test?
Use one variable at a time. Try the same serving size, same timing, and same meal context for regular milk, lactose-free milk, and one unsweetened non-dairy alternative.
For a detailed comparison of specific products and strains, see Do You Need Lactase With Lactose-Free Milk?.
What is the practical next step?
If lactose-free milk still causes symptoms, stop treating lactose as the only possible variable. Write down the brand, portion, fat level, timing, meal context, and exact symptom pattern for one to two weeks. Compare lactose-free cow’s milk with one non-dairy alternative and one lower-fat or smaller-serving dairy option if tolerated. Keep coffee, cereal, protein powder, bedtime, and meal size as consistent as possible during each comparison. Note whether symptoms are lower-gut, upper-gut, skin-related, breathing-related, or whole-body, because those patterns point in different clinical symptom directions. If symptoms repeat despite careful testing, or if red flags appear, bring the log to a clinician. The goal is not to prove that lactose-free milk is “bad.” The goal is to identify whether lactose, dairy protein, fat, volume, reflux timing, additives, or another digestive pattern explains the reaction.