Digestion can feel different every week because gut motility, meal timing, fiber intake, hydration, stress, sleep, hormones, medications, and recent infections all shift how fast food and gas move through the gastrointestinal tract. A weekly change is not automatically random. It is often a pattern created by repeatable inputs.
How did we evaluate weekly digestion changes?
We evaluated weekly digestion changes by separating normal digestive variability from warning signs that need medical attention. We prioritized NIDDK anatomy and physiology references, peer-reviewed reviews on circadian rhythm and gut motility, and clinical references on the gastrocolic reflex because those sources explain mechanisms rather than anecdotes. We excluded detox language, microbiome-reset promises, and single-cause explanations because this cold-stage guide is educational only. The limitation is personal context: bowel rhythm can change from harmless routine shifts, but persistent pain, bleeding, fever, unexplained weight loss, or major new bowel changes require a clinician. This article focuses on pattern recognition, not diagnosis, and uses plain categories that help people compare one week with the next. It also treats normal variation as data, not as proof that something is wrong right now today in daily life patterns.
Why does digestion change even when meals look similar?
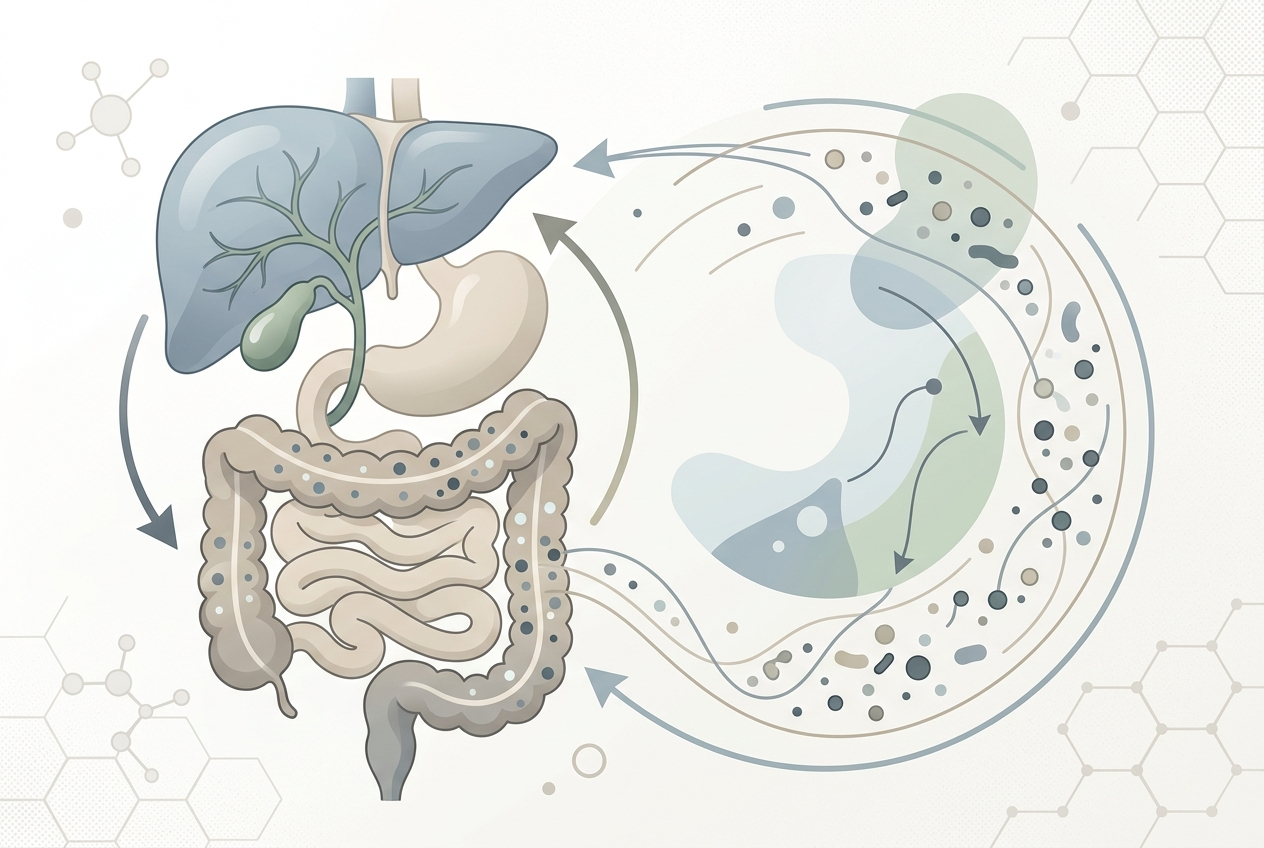
Digestion changes because the gastrointestinal tract responds to more than food ingredients. The NIDDK digestive-system guide explains that nerves and hormones help control digestion while organs move food, break it down, absorb nutrients, and form stool. Two salads can behave differently if one is eaten after poor sleep, low water intake, travel, extra coffee, a stressful workday, or a skipped breakfast. Fiber type also matters: beans, onions, wheat, apples, oats, and leafy greens can affect stool form and gas differently because they contain different fermentable carbohydrates and textures. Fat slows gastric emptying for some meals, while large meals stretch the stomach more than small meals. Weekly digestion therefore reflects meal composition, nervous-system state, hydration, and timing together, not one isolated food. The same food can feel different when the body context changes slightly.
How does the gastrocolic reflex affect weekly bowel patterns?
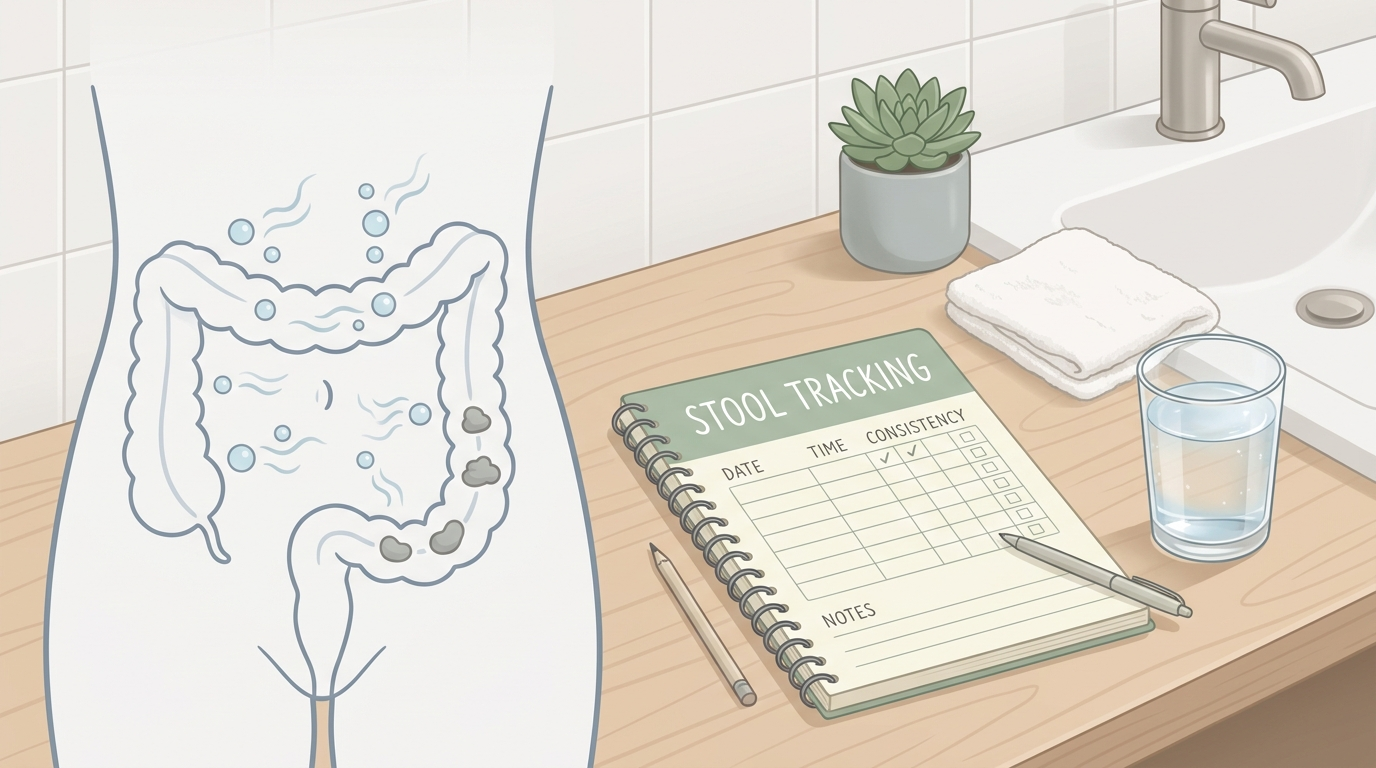
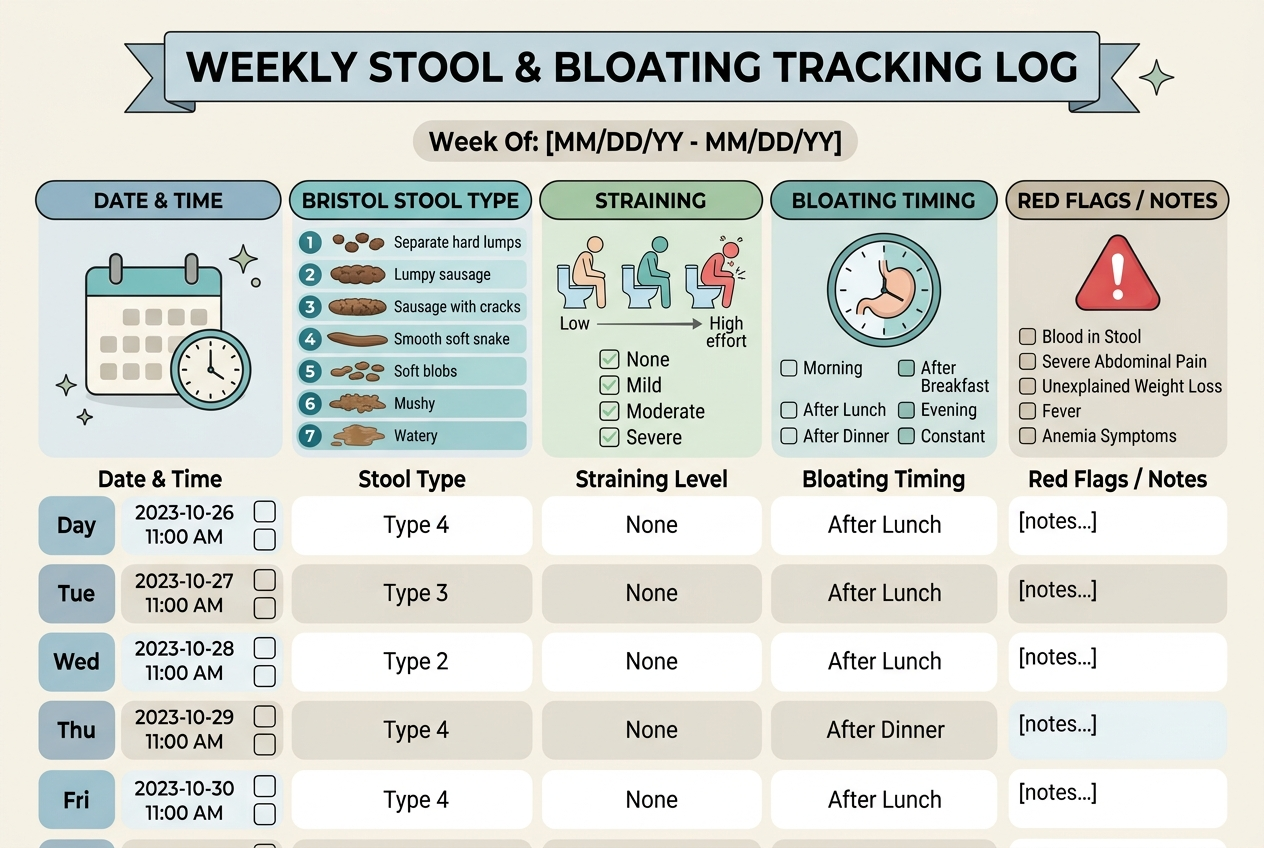
The gastrocolic reflex can make bowel urgency feel unpredictable, even when it follows a clear meal pattern. The NCBI Bookshelf review on the gastrocolic reflex describes it as a physiological reflex that increases lower gastrointestinal motility after food stretches the stomach. A bigger breakfast, a high-fat brunch, or a fast meal can create a stronger colon response than a small snack. Coffee can add a separate stimulation cue for some people. If weekday breakfasts are rushed and weekend meals are larger, bowel timing may shift every week without a new disease process. The practical pattern is timing: symptoms that appear soon after meals often track stomach stretch, meal size, fat content, caffeine, and routine. A simple log should record when eating starts, when urgency appears, and what changed that day, including portion size and pace.
Why do sleep, travel, and schedule changes affect the gut?
Sleep, travel, and schedule changes affect the gut because digestive organs follow circadian timing. A review in Cellular and Molecular Gastroenterology and Hepatology reports that circadian rhythms regulate gastrointestinal physiology, including motility, digestion, absorption, and electrolyte balance. Late dinners, shift work, jet lag, irregular wake times, and weekend sleep-ins can shift when the bowel is ready to move. Travel adds dehydration, different foods, long sitting, and bathroom avoidance, which can slow stool movement. A person may then swing from constipation during travel to looser stools after returning to normal meals and coffee. This is not proof that the gut is fragile. It shows that the gut acts like a timed system. Regular meals, morning light, fluid intake, and movement often reveal whether schedule disruption is the main driver behind the weekly change pattern.
Can hormones or the menstrual cycle change digestion week to week?
Hormones can change digestion week to week, especially across the menstrual cycle. A review on irritable bowel syndrome and the menstrual cycle reports that menstrual-cycle phase can affect bowel habits and may increase diarrhea, bloating, and abdominal pain in some people, with stronger effects in people who already have gut sensitivity. Prostaglandins, progesterone, estrogen shifts, pain, sleep disruption, and food-craving changes can all alter bowel rhythm around the same calendar window each month. The pattern can look weekly if symptoms begin before bleeding, peak during the first days, and settle afterward. A cycle-aware log is useful because it separates food blame from timing. The goal is not to label every symptom hormonal; it is to notice whether predictable dates change stool form, gas, urgency, or constipation in a repeatable way across months and cycles.
What is the safest way to find the pattern?
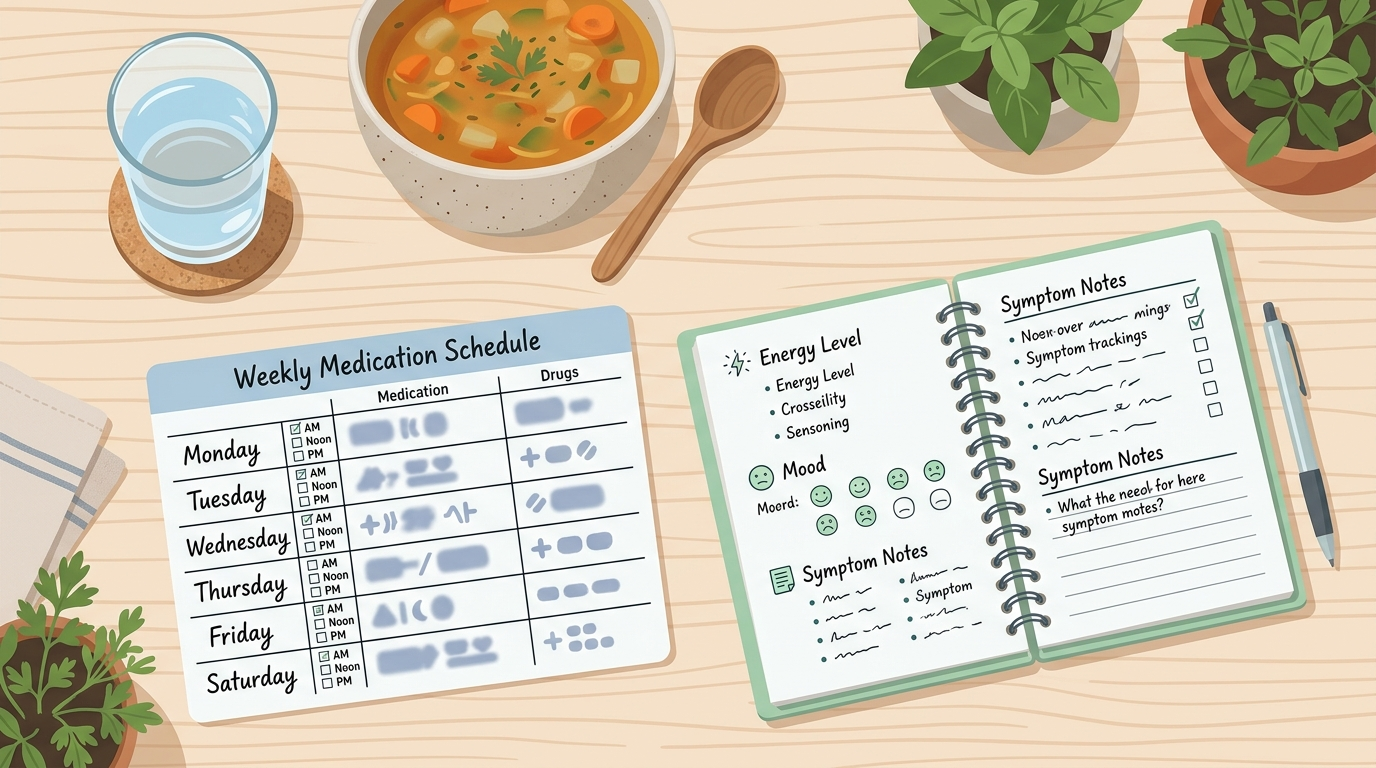
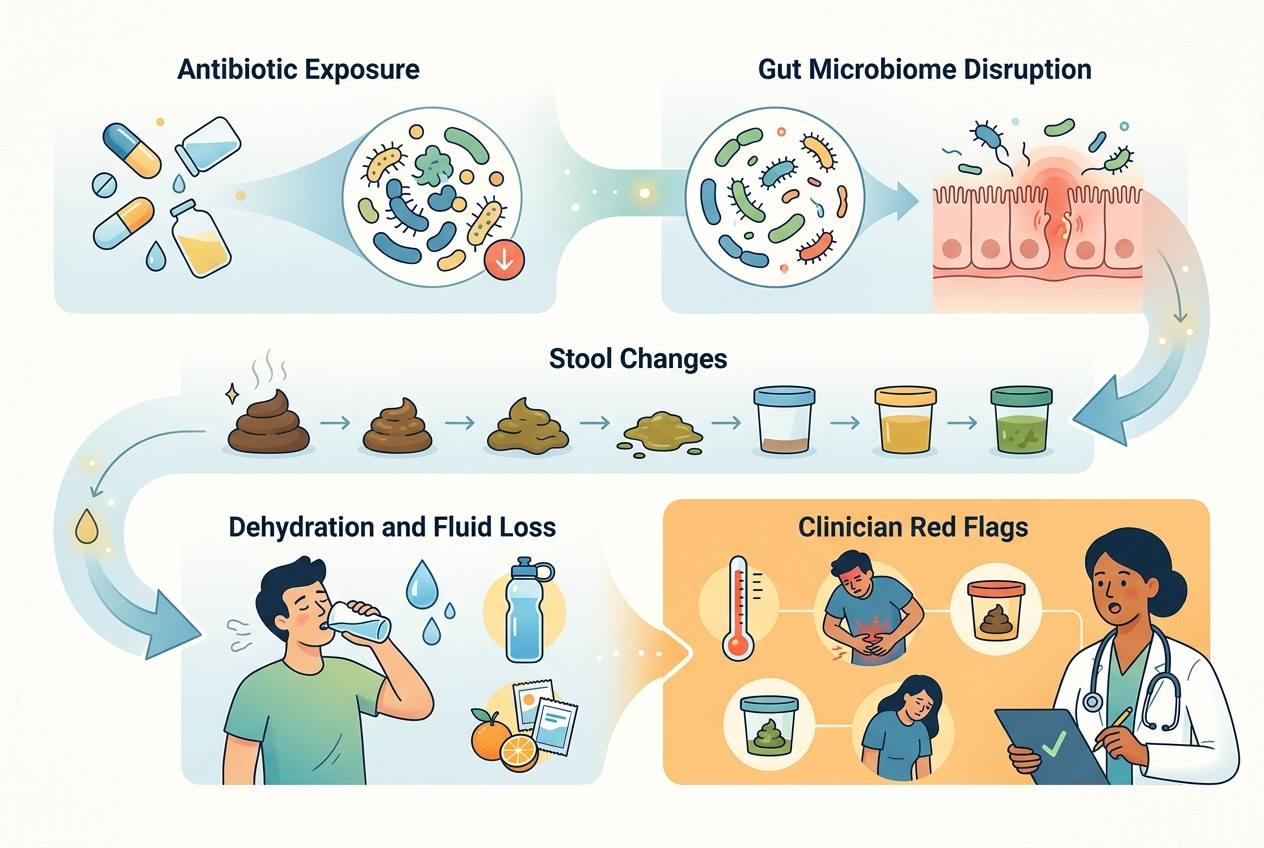
The safest way to find the pattern is to track a small set of variables for two weeks without changing everything at once. Record meal timing, fiber-heavy foods, dairy, alcohol, caffeine, water intake, sleep duration, stress level, bowel timing, stool form, and any new medication or routine change. Avoid starting a strict elimination diet from one bad week because removing many foods can hide the real signal and create nutrition gaps. The better test changes one variable for three to four days while the rest of the routine stays stable. Red flags change the plan: blood in stool, black stool, persistent vomiting, fever, severe dehydration, unintended weight loss, nighttime diarrhea, or new symptoms after age 45 deserve medical guidance. Pattern tracking works best for mild, recurring variability; it is not a substitute for care when symptoms are severe or escalating.
What questions do people ask about digestion changing every week?
Is it normal for bowel movements to vary by week?
Some variation is normal because sleep, stress, hydration, meal timing, and fiber intake change from week to week. A stable person can still have different stool timing after travel, large meals, or a disrupted schedule.
Why do weekends change my digestion?
Weekends often change wake time, coffee timing, alcohol intake, restaurant meals, movement, and bathroom routine. Those inputs can shift the gastrocolic reflex, stool water content, and gas production.
Can stress really change digestion that fast?
Stress can change gut sensation, motility, appetite, and bathroom timing through nervous-system signaling. The effect can appear quickly, especially when stress also changes coffee, sleep, and meal choices.
Should I blame one food when symptoms appear?
One food is possible, but a single meal is not enough evidence. Repeated timing, portion size, preparation, and co-factors matter more than one isolated bad day.
How long should I track symptoms?
Two weeks is usually enough to spot obvious timing patterns, and one full menstrual cycle is better for cycle-linked symptoms. Track lightly, because obsessive logging can make normal variation feel threatening.
When should I stop self-tracking and call a clinician?
Stop self-tracking if symptoms are severe, persistent, new, or paired with blood, fever, dehydration, vomiting, unexplained weight loss, or nighttime diarrhea. Those signs need medical judgment rather than spreadsheet detective work.
For a detailed comparison of specific products and strains, see Why Digestive Relief Feels Temporary and What to Compare Next.
What is the bottom line on weekly digestion changes?
Weekly digestion changes usually come from repeatable shifts in motility, timing, hydration, fiber, stress, sleep, travel, hormones, or recent illness. The pattern becomes clearer when meals, bowel timing, stool form, and schedule changes are logged together. If red flags appear, medical evaluation matters more than trying to force a pattern from incomplete notes alone at home.
Image prompts:
- Hero image: Calm editorial image of a weekly calendar beside simple meals, a water glass, walking shoes, and a sleep tracker, bright neutral health-education style, no brand logos. Alt text: Weekly digestion pattern calendar with meals, hydration, sleep, and movement cues.
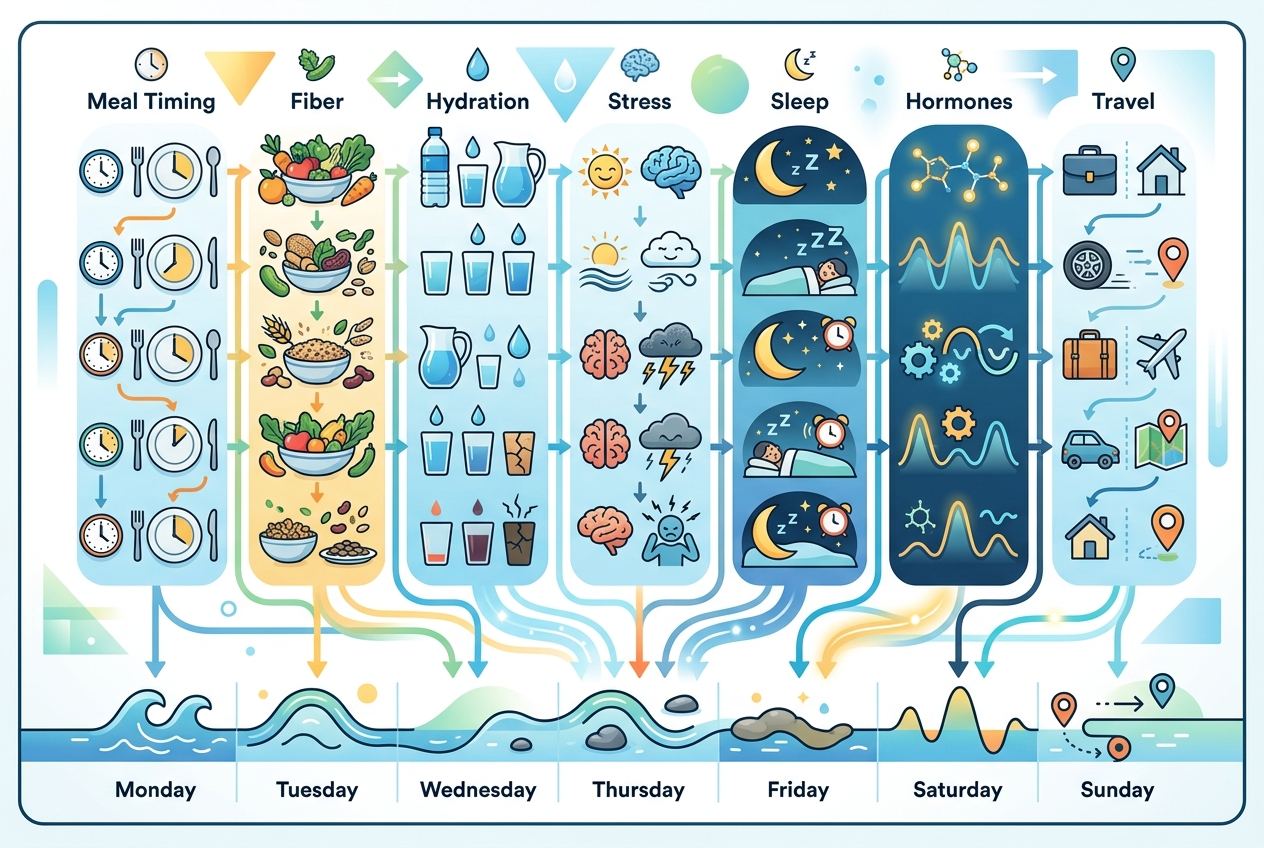
- Inline image: Clean infographic showing digestion inputs across a week: meal timing, fiber, hydration, stress, sleep, hormones, and travel, connected to bowel rhythm. Alt text: Diagram of weekly factors that can change digestion patterns.