Nexium may be helping if heartburn frequency, acid regurgitation, night waking, antacid rescue use, and meal-trigger recovery improve over 2 to 4 weeks. Progress is real when the same daily log shows fewer or milder reflux episodes, not just one good day. Persistent swallowing trouble, bleeding, weight loss, or chest pain needs clinician input.
How did we evaluate whether Nexium is helping?
This article evaluates Nexium progress by symptom trajectory, medication timing, safety signals, and clinician reassessment points. Medical references received priority when they came from government health resources, gastroenterology guidelines, drug-label sources, or peer-reviewed clinical guidance. The review excluded supplement comparisons, product recommendations, anecdotal forum claims, and brand-sponsored interpretations because a cold educational article should answer the reflux question without commercial bias. Evidence quality varies: guideline recommendations describe common clinical pathways, while an individual symptom log describes only one person’s pattern. Nexium is discussed as esomeprazole, a proton pump inhibitor, and not as proof that reflux is the only explanation for upper digestive discomfort. The method favors repeatable markers over impressions because memory exaggerates both good days and bad days. A clinician remains the right source for personalized medication duration, dose changes, alarm symptoms, and evaluation when symptoms persist or change.
What does Nexium change in reflux symptoms?
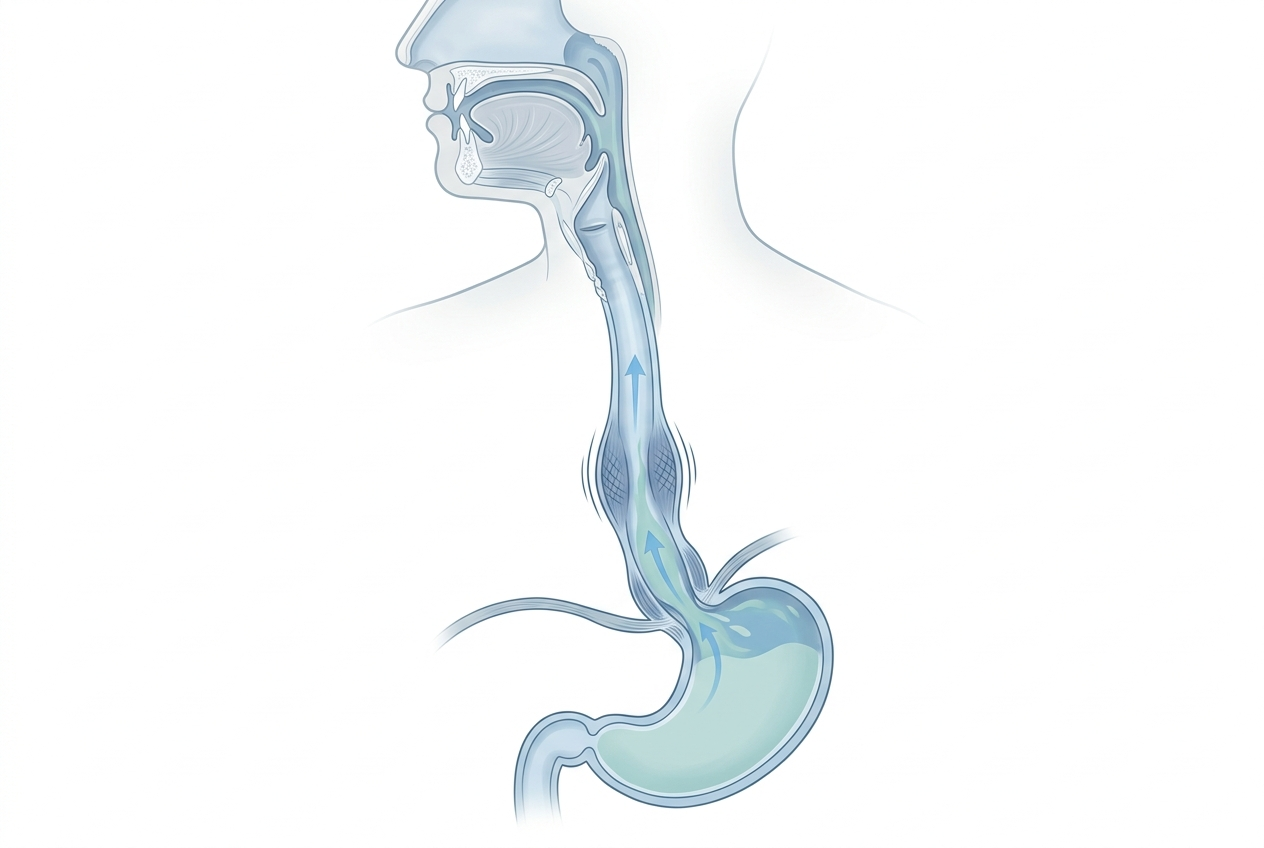
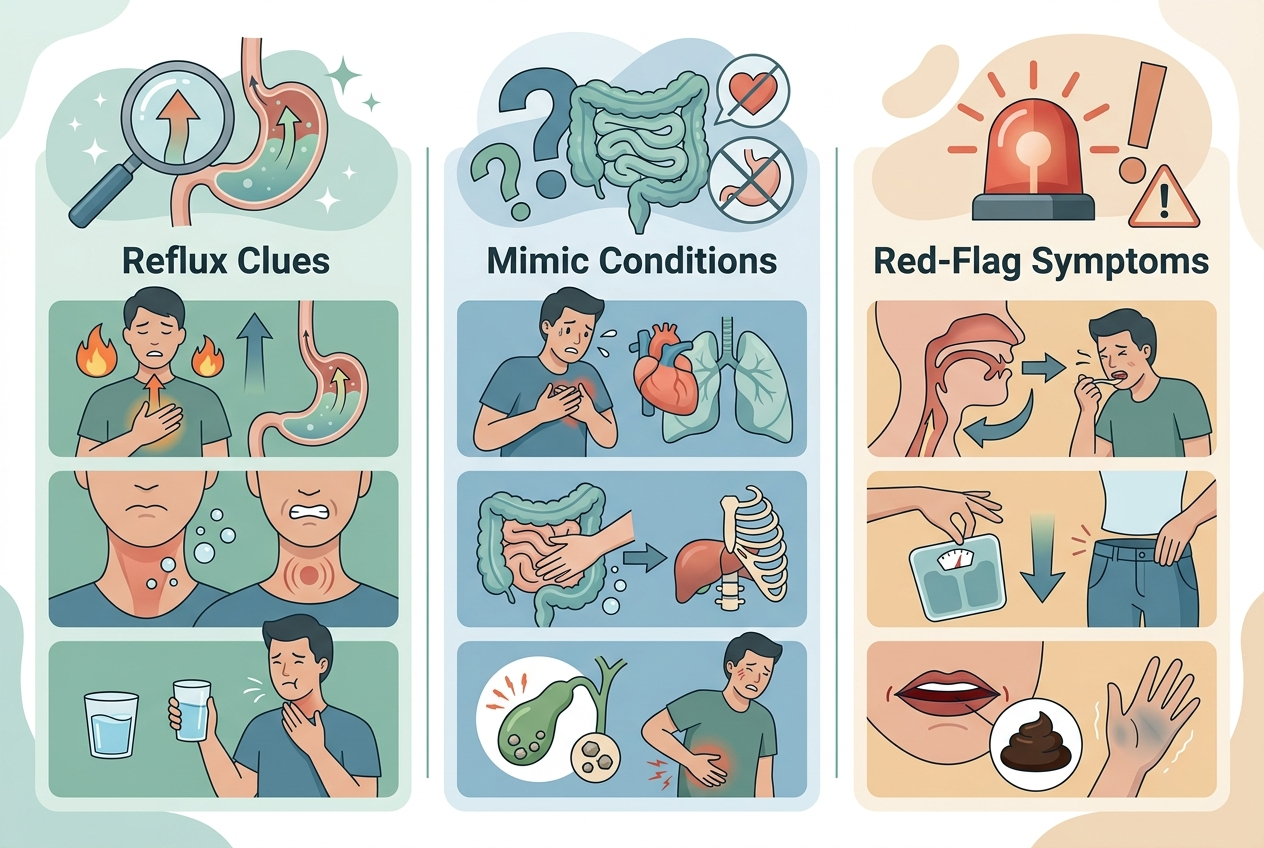
Nexium contains esomeprazole, a proton pump inhibitor that lowers gastric acid production by acting on the stomach acid pump. Lower acid exposure can reduce the burning sensation associated with acid reflux, but lower acidity does not stop every reflux event from moving upward. The MedlinePlus esomeprazole monograph lists esomeprazole as a medicine used for conditions involving excess stomach acid, including GERD, and gives practical timing and safety instructions. The useful progress markers are symptom-based: fewer heartburn episodes, less sour regurgitation, fewer nighttime awakenings, fewer rescue antacid doses, and less post-meal discomfort. A consistent meal-timing pattern makes those markers easier to interpret. Severity still needs daily tracking. Nexium is less informative when chest pressure, swallowing difficulty, vomiting, bleeding, or unintended weight loss appears. Those symptoms require clinician guidance because acid suppression does not identify the cause.
What signs show reflux progress is real?
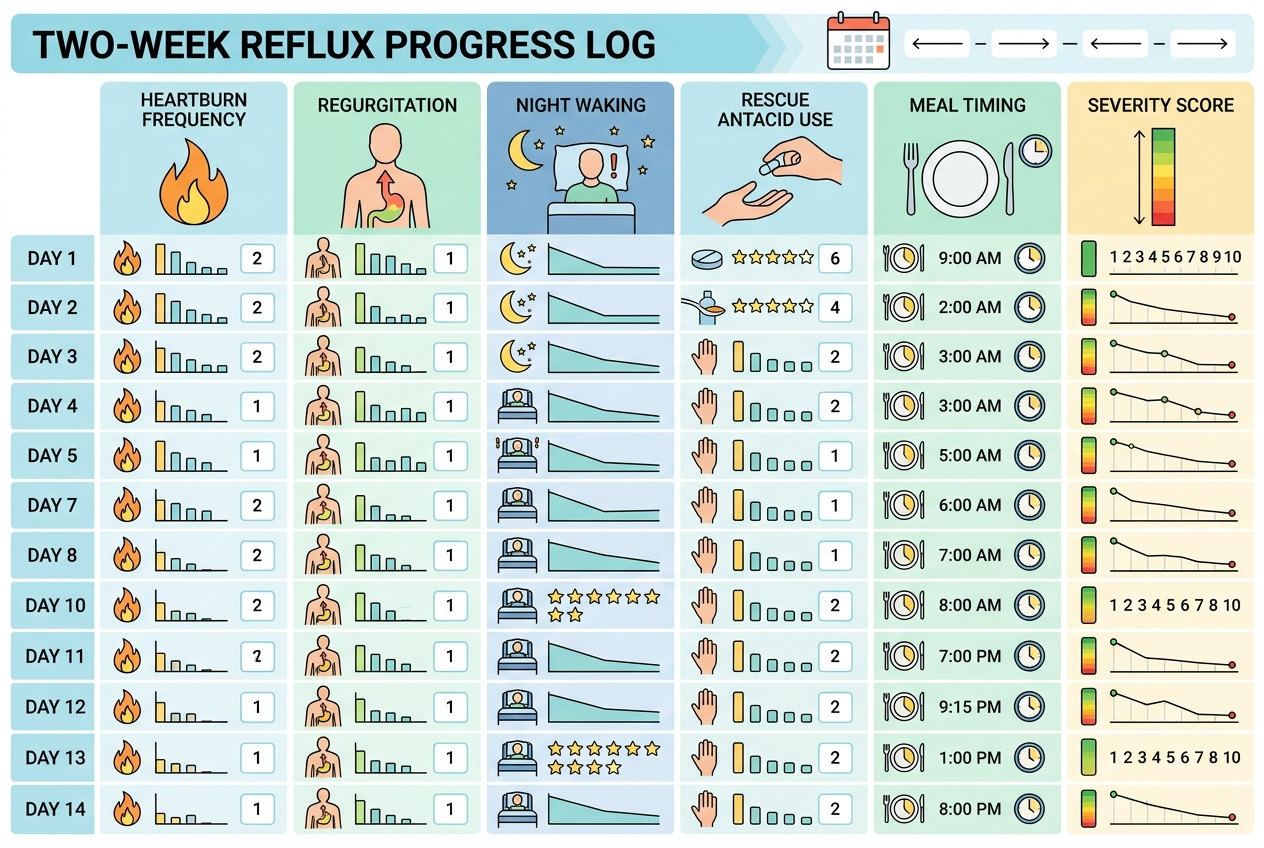
Real reflux progress means the same measurements improve across repeated days. A good week matters more than a good morning. Track heartburn frequency, regurgitation frequency, nighttime waking, rescue antacid use, meal-triggered discomfort, and the time needed for symptoms to settle after eating. A simple 0-to-10 severity score helps separate true improvement from memory bias. A reliable pattern usually shows fewer episodes, lower severity, shorter duration, or less disruption to sleep and meals. The NIDDK adult acid reflux and GERD resource describes heartburn and regurgitation as common reflux symptoms, so those two markers deserve special attention. Progress is weaker when symptoms move around without becoming less frequent or less disruptive. Progress is also unclear when food avoidance becomes extreme, because restriction can hide symptoms without showing whether the underlying pattern improved. The cleanest comparison uses the same meals, timing, and rating scale.
How long should progress take before reassessing?
A common reassessment window is several weeks, not several doses. The American College of Gastroenterology GERD guideline recommends an 8-week once-daily proton pump inhibitor trial before a meal for adults with classic heartburn and regurgitation when alarm symptoms are absent. That guideline supports structured reassessment rather than endless guessing. Earlier check-ins make sense when symptoms worsen, side effects appear, medication timing is uncertain, or alarm symptoms develop. Nexium timing matters because proton pump inhibitors usually work best when taken before a meal, according to medication guidance. Progress after 2 to 4 weeks can be meaningful, but incomplete progress should be interpreted against the full plan, dose instructions, and symptom log. A calendar date keeps the plan from drifting. A clinician can decide whether the issue is timing, duration, adherence, reflux phenotype, or another explanation.
What signs mean Nexium may not be enough?
Nexium may not be enough when reflux-like symptoms persist despite correct timing, consistent use, and a reasonable observation window. It also may not be the right answer when symptoms do not match classic heartburn or sour regurgitation. Alarm features change the priority: trouble swallowing, painful swallowing, vomiting blood, black stools, unexplained anemia, unintended weight loss, persistent vomiting, or severe chest pain should prompt urgent clinician input. The ACG GERD guideline highlights alarm symptoms as reasons for further evaluation rather than routine symptom-only management. Chest pain deserves extra caution because heart-related problems can mimic reflux sensations. A symptom log can show whether Nexium changed acid-related discomfort, but a log cannot confirm the cause. Persistent symptoms need a clinician’s review of medication timing, other medicines, diet pattern, stress, sleep position, and possible non-reflux causes. New or escalating symptoms deserve faster review than stable, mild symptoms.
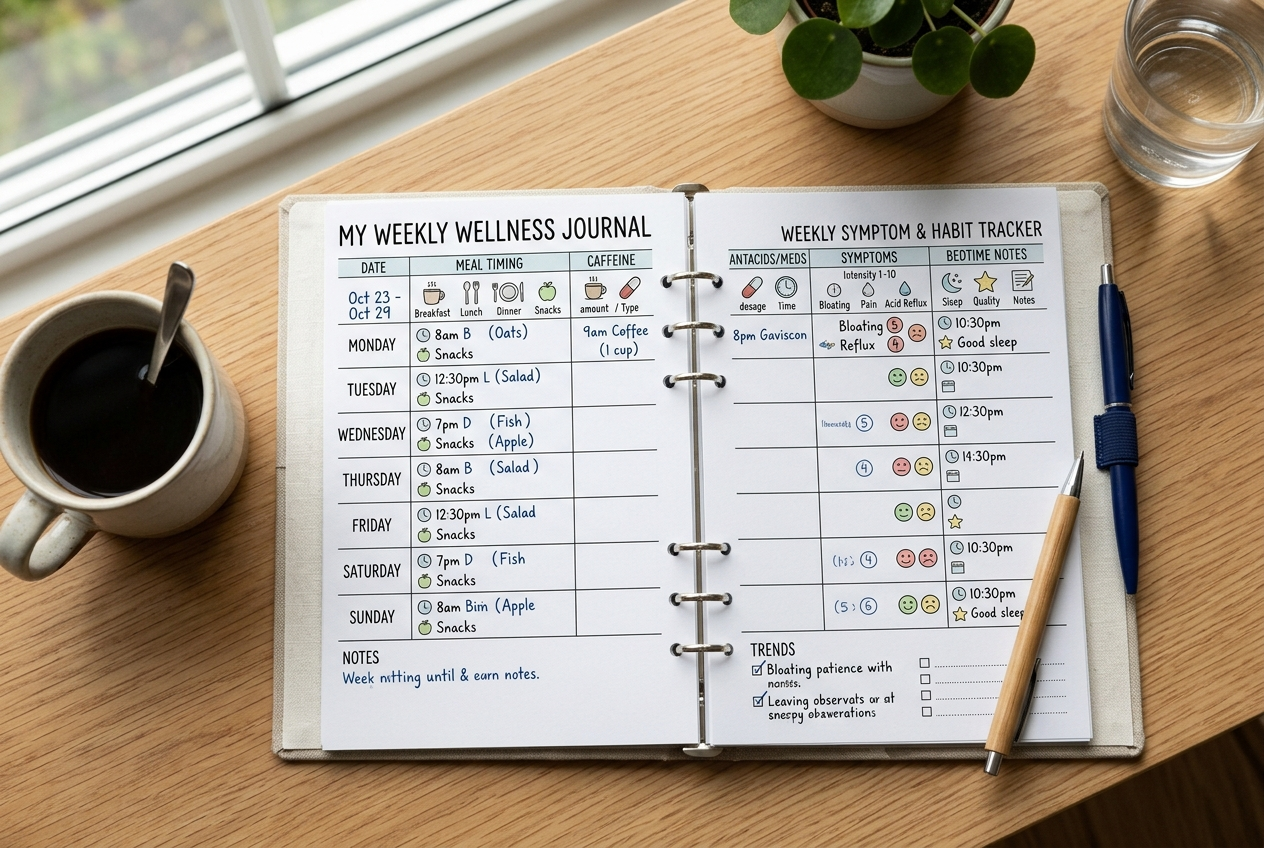
How should you track progress without fooling yourself?
A reflux progress log should measure the same signals every day for at least 2 weeks. Record Nexium timing, first meal timing, heartburn episodes, regurgitation episodes, nighttime waking, rescue antacid doses, trigger meals, alcohol, caffeine, late eating, stress level, and symptom severity from 0 to 10. Use the same scale each day because changing the scale creates false progress. Compare weekly averages, not isolated highs or lows. Real improvement appears as lower frequency, lower severity, shorter duration, or fewer rescue behaviors. Add one notes line for unusual events, such as travel, missed doses, large late meals, or new medications. Do not change several lifestyle variables at once if the goal is clarity. A cleaner tracking period gives the clinician better information and helps separate medication response from natural day-to-day variation. A spreadsheet, paper calendar, or phone note can work if entries stay consistent.
What should you ask a clinician before changing Nexium?
Ask a clinician whether the Nexium dose, timing, duration, and follow-up plan match your symptom pattern. Ask whether the medication should be taken before breakfast, before dinner, or in another schedule based on your specific prescription. Ask what symptom threshold should trigger reassessment before the planned endpoint. Ask whether other medicines, pregnancy, kidney concerns, magnesium concerns, bone-health risk, or infection history changes the safety discussion. The FDA prescribing information for Nexium lists dosing, warnings, precautions, and drug-interaction details that clinicians use when weighing duration and monitoring. Ask how long to keep the symptom log and which changes matter most. Do not stop, restart, double, or taper prescription esomeprazole based only on internet guidance. A short appointment can turn a vague question, “Is this helping?” into a specific plan with dates, markers, and next steps.
For a detailed comparison of specific products and strains, see How to Tell If a Probiotic Is Helping: Keep, Switch, or Stop?.
What are the most common questions about Nexium progress?
Can Nexium help if symptoms are not classic heartburn?
Nexium is most informative when symptoms resemble acid-related heartburn or sour regurgitation. A clinician should evaluate symptoms such as chest pressure, swallowing trouble, persistent nausea, or unexplained weight loss because those patterns need a broader review.
Is one symptom-free day enough evidence of progress?
One symptom-free day is encouraging, but it is weak evidence by itself. Weekly averages across heartburn frequency, regurgitation, night waking, and rescue antacid use give a more reliable signal.
Should Nexium stop all reflux episodes?
Nexium lowers stomach acid production; it does not create a physical barrier that blocks every reflux event. A person can have less acidic reflux and still notice pressure, burping, throat symptoms, or regurgitation.
What if symptoms improve but return at night?
Night symptoms can reflect late meals, sleep position, alcohol, larger evening portions, or medication timing. A clinician can review whether the pattern fits reflux management, another upper digestive issue, or a medication-schedule problem.
What if Nexium works only when I avoid many foods?
Heavy restriction can make progress hard to interpret because fewer triggers may hide symptoms. A structured log should separate medication timing, food pattern, meal size, and symptom severity before drawing conclusions.
Can I change the dose if progress feels slow?
Do not change prescription esomeprazole dose or schedule without clinician guidance. Dose changes depend on the reason for use, symptom pattern, safety factors, other medicines, and the planned reassessment window.
When should I seek urgent help?
Seek urgent medical help for severe chest pain, vomiting blood, black stools, fainting, trouble swallowing, or symptoms that feel different from your usual reflux pattern. These signs require prompt human evaluation, not home tracking.