Chest pain after eating can come from reflux, esophageal spasm, trapped gas, gallbladder pain, muscle strain, anxiety, or heart-related causes. Because heart pain and digestive pain can overlap, new, severe, persistent, crushing, unexplained, or spreading chest pain deserves urgent medical evaluation before assuming it is indigestion.
How did we evaluate chest pain that comes after eating?
We evaluated post-meal chest pain by separating emergency-risk patterns from common digestive patterns. Medical references from Mayo Clinic, NIDDK, MedlinePlus, Cleveland Clinic, and the American College of Gastroenterology carried more weight than anecdotal symptom descriptions. We prioritized signs that help a person decide whether to seek care, track meal-related patterns, or discuss reflux and esophageal causes with a clinician. We excluded product recommendations because a cold educational article should explain the symptom pattern without pushing antacids, remedies, or any brand.
When is chest pain after eating an emergency?
Chest pain after eating is an emergency when the pain is new, severe, unexplained, persistent, pressure-like, or paired with shortness of breath, sweating, faintness, nausea, jaw pain, back pain, shoulder pain, or arm pain. Mayo Clinic says severe chest pain or new unexplained chest pain or pressure lasting more than a few moments should prompt emergency medical care. MedlinePlus warns that chest pain with shortness of breath or pain in the jaw or arm can signal a heart problem. A meal trigger does not rule out the heart because heart symptoms can appear during rest, stress, exertion, or digestion. The safest rule is simple: evaluate the dangerous possibilities first. After a clinician has considered heart-related causes, digestive explanations such as reflux, esophageal irritation, or gas become more reasonable to explore.
Why can reflux cause chest pain after meals?
Reflux can cause post-meal chest pain when stomach contents move upward into the esophagus and irritate tissue behind the breastbone. The NIDDK reflux overview describes heartburn and regurgitation as common GER and GERD symptoms, and those symptoms often cluster after larger meals, trigger foods, lying down, or bending. Cleveland Clinic explains that acid reflux can feel like burning chest pain near the sternum, which is why people often confuse reflux pain with heart pain. Reflux pain may feel burning, sour, bitter, or pressure-like, but symptom feel alone cannot prove the cause. A clinician may ask about timing, regurgitation, swallowing symptoms, medication use, pregnancy, smoking, alcohol, and meal size. Reflux becomes more likely when episodes repeatedly follow meals and improve with upright posture, but it is still not a self-diagnosis.
What non-heart digestive causes can mimic post-meal chest pain?
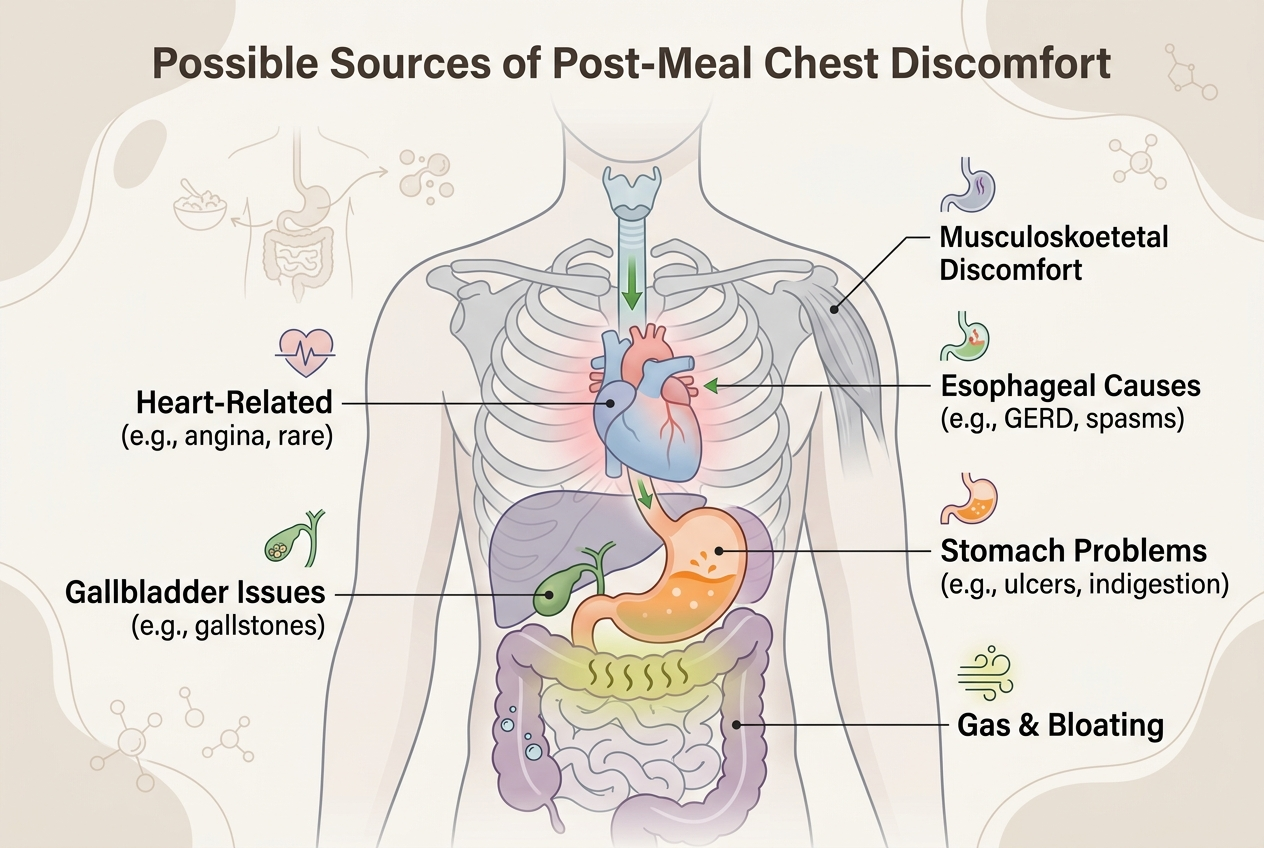
Several digestive and nearby causes can mimic chest pain after eating. Esophageal spasm can create squeezing pain because the esophagus runs through the chest. Swallowing problems, pill irritation, or food sticking can create pain that feels centered behind the breastbone. Gas distension can push discomfort upward, especially after carbonated drinks, fast eating, large meals, or constipation. Gallbladder pain can follow fatty meals and may sit in the upper abdomen or right upper side while radiating toward the back or shoulder. Muscular chest-wall strain can feel worse with movement or pressure on the ribs. Anxiety can amplify normal digestive sensations and chest tightness, but anxiety should not be used to dismiss new chest pain. The American College of Gastroenterology notes that GERD-related chest pain can resemble angina, so cardiac evaluation comes before assuming the esophagus is responsible.
What patterns are useful to track before a medical visit?
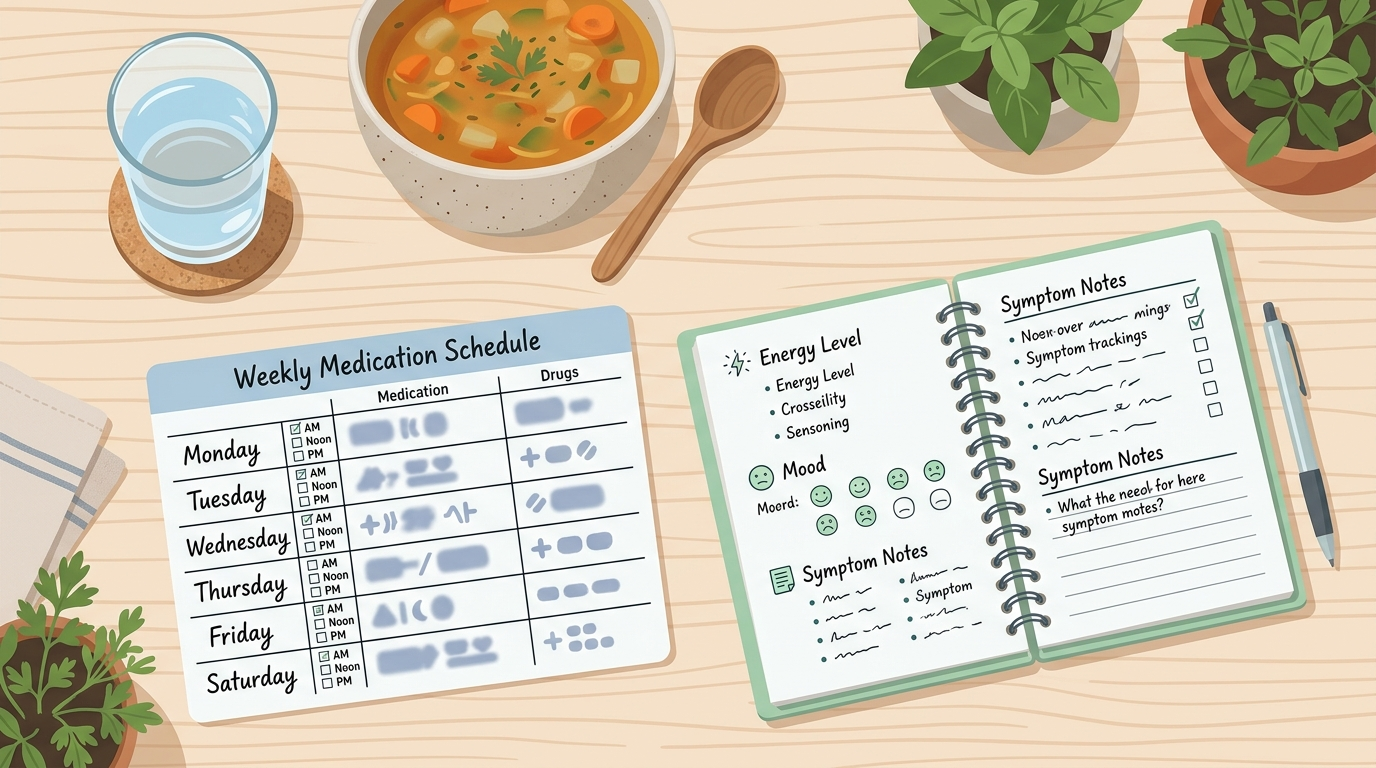
A post-meal chest-pain diary should track time of onset, meal size, trigger foods, alcohol, caffeine, carbonated drinks, posture, exertion, stress, bowel pattern, medications, and how long the pain lasts. The diary should also record whether symptoms include sour regurgitation, trouble swallowing, nausea, sweating, shortness of breath, dizziness, or pain spreading beyond the chest. This pattern helps a clinician separate reflux-like episodes from exertional, cardiac, biliary, muscular, medication-related, or anxiety-linked patterns. A practical diary uses one line per episode: meal, time, pain location, intensity from 0 to 10, associated symptoms, and what changed it. Avoid testing multiple fixes at once because that makes the pattern harder to read. If chest pain is severe, new, or unexplained, tracking should wait until urgent causes have been evaluated.
What should you avoid doing when chest pain follows food?
Do not assume chest pain is harmless because it starts after food. Do not drive yourself to urgent care during severe chest pressure, shortness of breath, faintness, or spreading pain. Do not use repeated antacids, baking soda, alcohol, or extreme fasting as a substitute for evaluation. Do not keep exercising through chest pain to “test” whether it is digestive. Do not ignore swallowing trouble, vomiting blood, black stools, unintentional weight loss, persistent vomiting, or pain that wakes you from sleep. The American College of Gastroenterology reflux resource says people should not assume chest pain is esophageal until a physician has evaluated potential heart causes. The safest next step depends on severity: emergency help for red flags, medical follow-up for recurrent unexplained episodes, and tracking for mild repeat patterns after danger signs are absent.
What questions do people ask about chest pain after eating?
Can heartburn feel like chest pain?
Yes. Heartburn can feel like burning pain behind the breastbone, especially after meals or lying down. The problem is that heart-related pain can overlap, so new or unexplained chest pain should not be labeled heartburn without appropriate evaluation.
Can gas cause chest discomfort after eating?
Gas can cause pressure, bloating, belching, and upper abdominal discomfort that may feel close to the chest. Gas should not be blamed for crushing, spreading, severe, or unexplained chest pain.
Why does chest pain happen after a large meal?
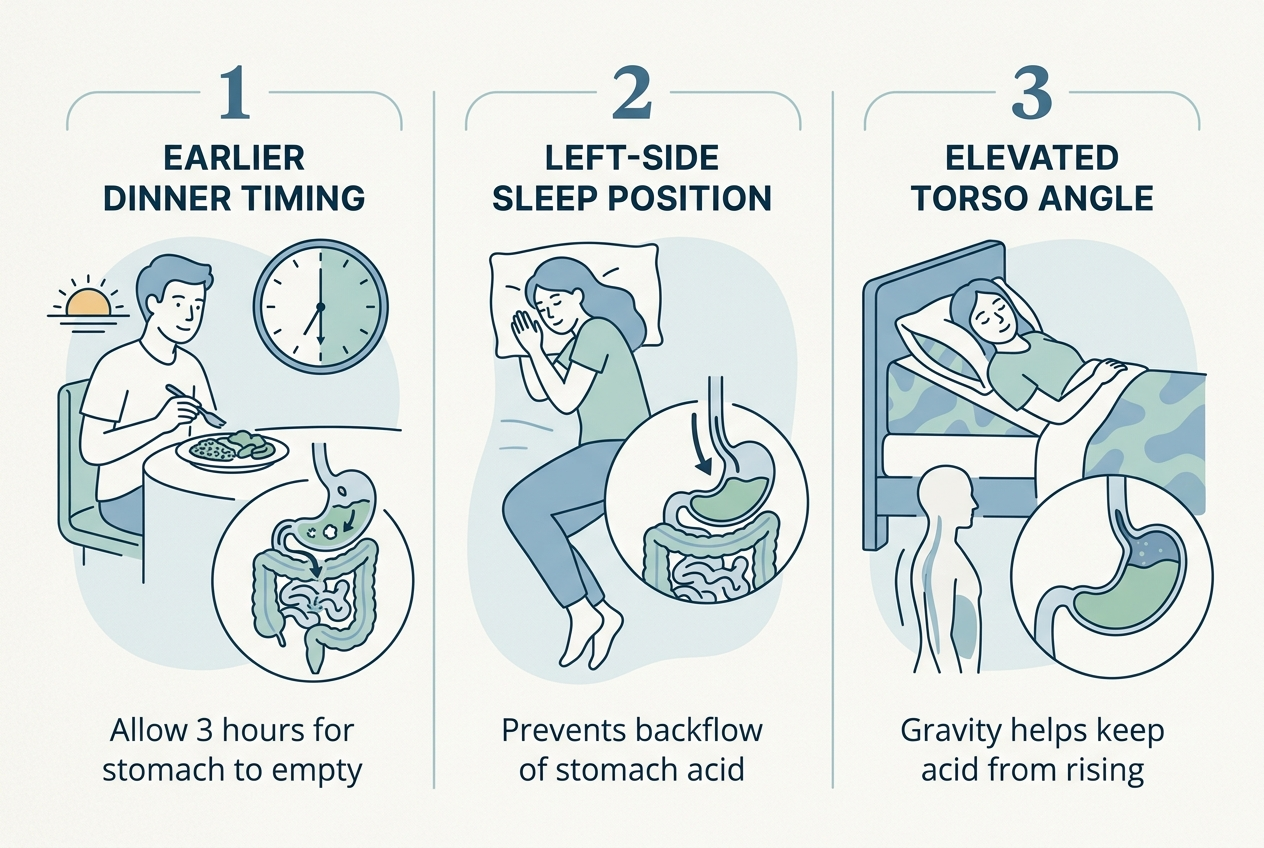
A large meal can increase stomach pressure, reflux risk, belching, and upper abdominal distension. Fatty meals can also slow stomach emptying for some people, which may make reflux-like symptoms more noticeable.
Is chest pain after eating always GERD?
No. GERD is one possible explanation, but heart conditions, esophageal spasm, gallbladder issues, muscle strain, anxiety, medication irritation, and swallowing disorders can also fit parts of the pattern.
Should I lie down if my chest burns after food?
Lying down can worsen reflux-like symptoms because gravity no longer helps keep stomach contents down. If the pain is new, severe, pressure-like, or paired with emergency symptoms, position changes are not enough; seek urgent help.
When should I call a doctor instead of waiting?
Call a clinician for recurrent post-meal chest pain, unexplained episodes that resolve, swallowing trouble, persistent reflux symptoms, vomiting, weight loss, black stools, or pain that keeps returning. Call emergency services for severe, new, persistent, spreading, or breathing-related chest pain.
What is the bottom line on chest pain after eating?
Chest pain after eating can be digestive, but it is not automatically digestive. Reflux, gas, esophageal spasm, gallbladder pain, muscle strain, and anxiety can all follow meals, while heart-related pain can overlap with indigestion. Treat red flags as urgent, then use pattern tracking and medical follow-up to sort out repeat meal-related episodes.
Image prompts:
- Hero image: Calm educational scene with a dinner plate, water glass, upright chair, and a simple symptom diary on a kitchen table; neutral health editorial style, no products, no logos, no emergency imagery. Alt text: Meal and symptom diary used to track chest pain after eating.
- Inline image: Clear medical-style infographic showing possible sources of post-meal chest discomfort: heart, esophagus, stomach, gas, gallbladder, and chest wall; neutral colors, no frightening imagery. Alt text: Diagram of possible causes of chest pain that comes after eating.