Allergies can make acid reflux feel worse when nasal drainage, coughing, throat clearing, chest pressure, or sleep disruption irritates the upper airway. Allergies do not usually cause reflux by themselves, but allergy flares can overlap with GERD symptoms and make throat burning, sour taste, hoarseness, or nighttime discomfort harder to interpret.
How did we evaluate acid reflux and allergies?
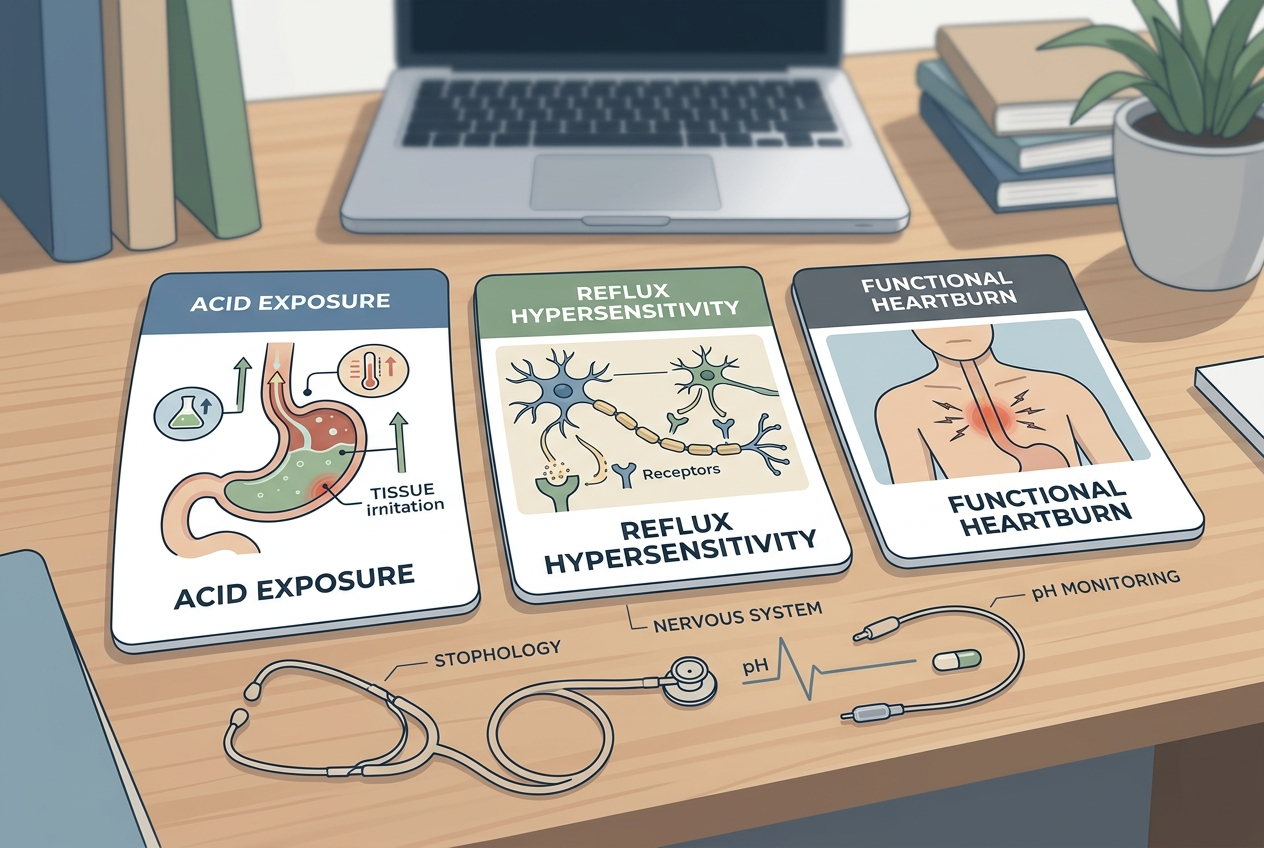
We evaluated acid reflux and allergies by separating digestive reflux mechanisms from upper-airway allergy symptoms. We prioritized NIDDK GERD guidance, Mayo Clinic reflux summaries, Cleveland Clinic postnasal drip education, and peer-reviewed research on reflux, cough, and airway symptoms. We excluded claims that seasonal allergies directly “cause GERD,” because the stronger evidence supports symptom overlap and irritation pathways rather than a single-cause model. We also excluded supplement, detox, and cleanse claims because this article is an educational explanation, not a product comparison. The practical question is pattern recognition: reflux tends to track meals, lying down, sour regurgitation, and burning, while allergy symptoms tend to track pollen, dust, pets, nasal itch, sneezing, and drainage. When both patterns appear together, a symptom diary can help separate triggers before a clinician adjusts medication, testing, or referral timing safely.
Can allergies make acid reflux symptoms feel worse?
Allergies can make reflux symptoms feel worse by increasing nasal drainage, throat clearing, coughing, and sleep fragmentation. Cleveland Clinic describes postnasal drip as mucus drainage that can cause coughing, throat clearing, sore throat, and hoarseness; those sensations can resemble laryngopharyngeal reflux. NIDDK explains that GERD can cause heartburn, regurgitation, chest discomfort, and swallowing-related symptoms when stomach contents move back into the esophagus. The overlap creates confusion because both conditions can irritate the throat without obvious stomach pain. Allergies may also worsen nighttime symptoms when congestion pushes mouth breathing, coughing, or poor sleep. That does not prove pollen or dust creates stomach acid. It means the airway and esophagus share symptom territory. The most useful clue is timing: allergy symptoms often follow exposure patterns, while reflux often follows meals, bending, alcohol, large portions, or lying down.
What symptoms point more toward reflux than allergies?
Symptoms point more toward reflux when burning rises behind the breastbone, sour or bitter fluid reaches the throat, burping follows meals, or discomfort worsens after lying down. Mayo Clinic lists heartburn after eating, regurgitation, upper abdominal or chest pain, trouble swallowing, and a sensation of a lump in the throat among GERD symptoms. Reflux also tends to worsen after large evening meals, peppermint, chocolate, fatty foods, alcohol, coffee, or tight waist pressure in susceptible people. Allergy symptoms point elsewhere when sneezing, itchy eyes, clear nasal drainage, seasonal timing, pet exposure, or dust exposure dominate the pattern. A mixed picture is common: a person may have allergic rhinitis and reflux during the same week. The diary question is not “which one is real?” The better question is which trigger starts first, which symptom lasts longest, and which change reliably helps.
What symptoms point more toward allergies than reflux?
Symptoms point more toward allergies when sneezing, nasal itching, watery eyes, clear runny nose, sinus pressure, and exposure-linked flares appear before throat symptoms. Allergic rhinitis often follows pollen seasons, indoor dust, mold, animals, or workplace irritants. Postnasal drip can create throat mucus, coughing, frequent swallowing, and morning hoarseness even when the stomach is not the main driver. Reflux can still coexist, especially if coughing increases abdominal pressure or poor sleep changes meal timing and caffeine intake. Antihistamines, decongestants, and nasal sprays can also change dryness, mucus thickness, or sleep quality, so medication timing belongs in the diary. A 2021 review in Frontiers in Medicine describes reflux and cough as a bidirectional clinical problem rather than a simple one-way cause. That nuance matters because throat symptoms can come from the nose, esophagus, lungs, medications, or several sources at once.
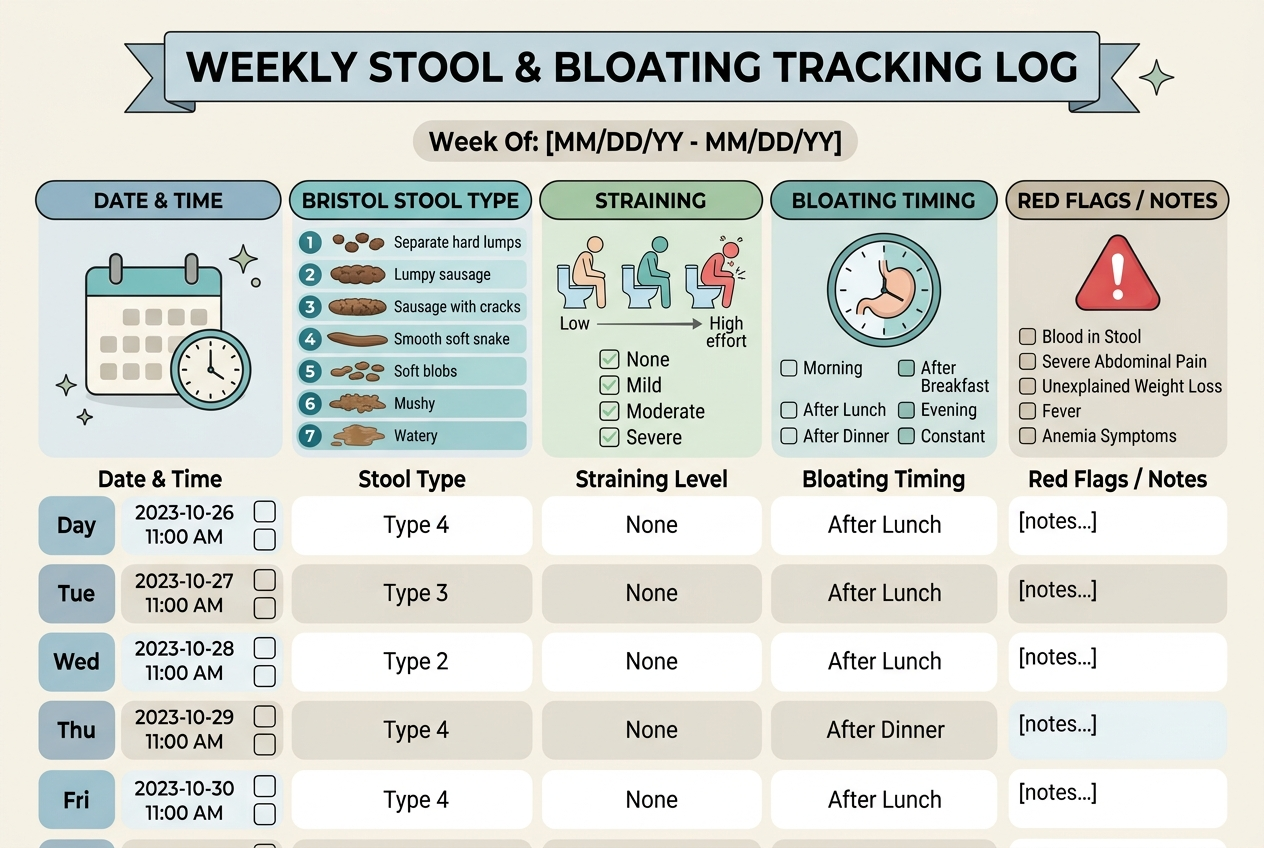
How can you track the difference at home?
A useful home log records meals, lying-down time, allergy exposure, nasal symptoms, throat symptoms, cough, medications, and sleep position for seven to fourteen days. Reflux clues include symptoms within two to three hours after meals, worse symptoms after bending or lying down, sour taste, and improvement with smaller evening meals. Allergy clues include symptoms after outdoor exposure, dusty rooms, pets, open windows, or high-pollen days, especially when sneezing and itchy eyes appear. Record medication timing because a new antihistamine, decongestant, proton-pump inhibitor, H2 blocker, or nasal steroid can change the pattern. Avoid changing everything at once; stacked changes make the signal unreadable. Red flags need medical care rather than diary experiments: chest pain with exertion, trouble swallowing, vomiting blood, black stools, unexplained weight loss, choking, severe shortness of breath, or persistent symptoms despite appropriate treatment.
What common mistakes make the overlap harder to solve?
The first mistake is treating every throat symptom as reflux. Postnasal drip, vocal strain, viral illness, asthma, medication dryness, and irritant exposure can also cause throat clearing or cough. The second mistake is treating every sour taste as allergies, because regurgitation after meals is a classic reflux clue. The third mistake is taking multiple new remedies at once, then losing the ability to identify the helpful or irritating change. The fourth mistake is ignoring meal size, alcohol, late snacks, caffeine, and sleep position while focusing only on pollen counts. The fifth mistake is delaying care when symptoms are severe, new, progressive, or paired with swallowing trouble. Reflux and allergies can overlap, but overlap does not make self-diagnosis reliable. A clinician can evaluate GERD, allergic rhinitis, asthma, sinus disease, medication side effects, and throat conditions when the pattern stays confusing.
What questions do people ask about reflux and allergies?
People usually ask whether allergies cause reflux, whether postnasal drip can mimic reflux, and whether allergy medicine can change digestive symptoms. The best answer is cautious: allergies can worsen throat irritation and cough, while reflux can irritate the throat and airway, so the symptom map overlaps. A diary helps identify whether meals, body position, pollen, dust, pets, or medication timing starts the flare. Medical evaluation matters when symptoms are persistent, severe, or associated with warning signs. People should also remember that reflux and allergies can both be present, so improvement in one system may not fully clear the other. The goal is not to force one label onto every symptom. The goal is to identify the dominant trigger, reduce obvious aggravators, and get medical guidance when the pattern does not make sense clinically anymore.
Can postnasal drip feel like acid reflux?
Yes, postnasal drip can cause throat clearing, cough, mucus sensation, hoarseness, and sore throat. Those symptoms can feel similar to laryngopharyngeal reflux, especially when classic heartburn is absent.
Can acid reflux cause allergy-like throat symptoms?
Reflux can cause throat irritation, cough, hoarseness, sour taste, and a lump-in-throat sensation. It does not cause pollen allergy, but it can create symptoms in the same throat and airway area.
Can antihistamines make reflux worse?
Some people notice dryness, thicker mucus, sleep changes, or altered eating patterns after antihistamines. That does not prove reflux is worsening, so tracking medication timing and symptoms is useful.
Why are symptoms worse at night?
Night symptoms can worsen because lying down favors reflux, while congestion and postnasal drip can also worsen in bed. Late meals, alcohol, and mouth breathing can add more irritation.
Should you treat allergies or reflux first?
The first target should be the clearest pattern. Exposure-linked sneezing and itchy eyes point toward allergy management, while meal-linked burning and regurgitation point toward reflux evaluation.
When should you see a clinician?
Seek medical care for trouble swallowing, chest pain, vomiting blood, black stools, unexplained weight loss, choking, severe shortness of breath, or symptoms that persist despite appropriate care. These signs need evaluation, not home sorting.
Sources: